

The “incredibly high” excess death rate in 2022 should be urgently investigated by the Government, Australia’s top actuarial body has said.
According to new analysis of Australian Bureau of Statistics (ABS) data by the Actuaries Institute, there were 15,400 excess deaths during the first eight months of the year, with around one third having no link to Covid.
This is 13% higher than expected, which is an “incredibly high number for mortality” according to Karen Cutter, spokeswoman for the institute’s COVID-19 Mortality Working Group. It is “not clear” what is driving the increase, she said. “Mortality doesn’t normally vary by more than 1-2%, so 13% is way higher than normal level.”
“I’m not aware [of anything comparable] in the recent past but I haven’t gone back and looked [historically]. They talk about the flu season of 2017 being really bad, and the mortality there was 1% higher than normal. So it’s well outside the range of normal.”
According to the raw data released by the Australian Bureau of Statistics, there were 128,797 deaths from January 1st to August 31st, which was 18,671 or 17% higher than the historical average. Of those, 7,727 or 41% were attributed to Covid, leaving 10,944 non-Covid excess deaths.
The reason for the difference between the raw ABS data and the actuary figures is that, unlike with ONS data in the U.K. which use a five-year average baseline, the actuaries use a modelled baseline for calculating excess deaths. This aims to take into account trends like an ageing and growing population and improving health outcomes. The actuaries acknowledge that, compared to using the 2015-19 baseline, this results in a higher baseline and thus fewer excess deaths.
The Actuaries Institute found that around 8,200 deaths, or just over half the excess, were due to Covid as underlying cause and a further 2,100 deaths were ‘with’ Covid as a contributory cause. They added the two together to give their final figure for non-Covid excess of 5,100, or around one third. Why they chose to include deaths where the underlying cause was not COVID-19 in the ‘Covid deaths’, and exclude them from the analysis of excess non-Covid deaths is not clear. Between that and the potentially mistaken raising of the baseline via modelling and the total number of excess deaths may be considerably and artificially diminished. The effect is to cut the proportion of excess deaths that are non-Covid almost in half, from 59% in the raw data to 33% in the actuaries’ analysis.
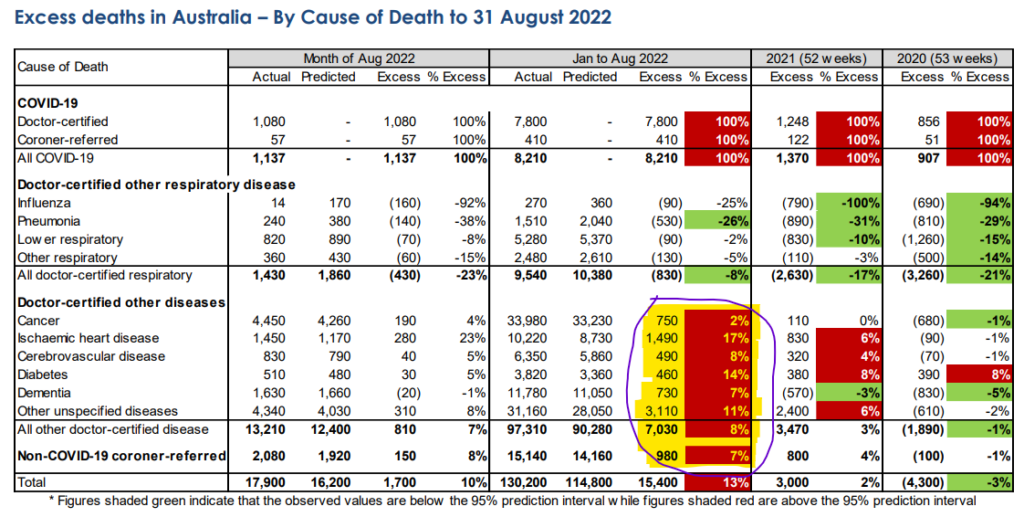
In any case, whatever the merits of these methods, the actuaries’ breakdown by cause of death is illuminating. According to the Actuaries Institute, 3,110 of the 8,010 non-Covid excess deaths were from “other unspecified” causes, which is 11% above the expected number, and 1,490 were from ischaemic heart disease, which is 17% above the expected number. Cerebrovascular disease (stroke) contributed 490 deaths, 8% above expected. Other cardiovascular causes were unfortunately not stated either by the actuaries or ABS, but were presumably included in the “other unspecified diseases”.
The actuaries state that deaths from respiratory disease other than COVID-19 have been significantly lower than expected throughout the pandemic (presumably owing to displacement by COVID-19). Cancer, diabetes, heart disease and stroke as a group have been the largest contributor to non-Covid excess deaths in 2021 and 2022, they state.
The high levels of excess deaths were seen across the country, with all states and territories having significant excess mortality in 2022. The exception was Northern Territory. Northern Territory has a population of just 250,000, and it is much younger than other states – the median age is six years lower, and just 5.6% are over 65, compared to 17.7% in New South Wales.
Excess deaths were seen in almost all age bands, though the percentage was higher in older groups. Karen Cutter said while the numbers of deaths in the 0-44 and 45-64 age bands were small, they were significantly higher than expected, particularly for females.
Ms. Cutter said it was “not clear what might be driving this” extreme increase in mortality, but partly it may be explained by the ‘dry tinder’ effect resulting from “less people dying from respiratory illness early on [compared with] what would have been pre-pandemic normal”.
She also suggested the deaths from diabetes, heart disease and stroke, were “highly related to Covid”, citing unspecified research.
She noted they are seeing “higher non-Covid deaths when there are Covid deaths”, such as in January and July, and suggested this could mean it is due to lack of access to healthcare or “more undiagnosed Covid than we know about”.
Vaccines blamed
The increase in heart and stroke deaths in particular has led many to suggest the Covid vaccines may be to blame. Earlier in the year, Australia’s Therapeutic Goods Administration (TGA) countered this claim, telling ABC Fact Check that it was “false and unscientific to automatically conclude that vaccines caused these deaths. There is no credible evidence to suggest that COVID-19 vaccines have contributed to excess deaths in Australia or overseas.”
This is untrue, of course: there is plenty of evidence from autopsies and other sources that the vaccines can kill, including silently and suddenly by triggering auto-immune attacks on the heart that can only be identified at autopsy. Their role thus cannot be ruled out without proper investigation.
Ms. Cutter even admitted that she “cannot prove” the vaccines are not involved, albeit as part of a denial that they are: “There is zero evidence that vaccines are causing these deaths as far as I’m concerned, but I cannot prove it.”
She argued that even if the 947 deaths in the TGA’s most recent safety report were confirmed to be linked to the vaccine (the TGA has to date only confirmed 14 as linked), it would only be a fraction of the total excess deaths. This doesn’t allow for under-reporting of vaccine injuries, though, of course.
She also claimed the timing of the excess deaths “doesn’t match with the vaccine rollout, and the age profile of people dying does not match with people who’ve been vaccinated”.
“Hardly any young people are dying,” she said. She also said there was no excess mortality in Western Australia in January and they were “just as vaccinated as the rest of the country”.
However, this doesn’t allow for people dying some weeks or months after their injection, perhaps due to an auto-immune attack triggered by a new challenge from the virus. It also doesn’t allow that vaccine deaths may be concentrated in older people with related co-morbidities. In addition, it overlooks that there are indeed excess deaths in younger people, as Ms. Cutter has acknowledged.
Zachary Stieber at Epoch Times has compiled a useful list of autopsy evidence from post-vaccine deaths.
In 2021, U.S. researchers reported two adults developed myocarditis within two weeks of COVID-19 vaccination, and they were unable to find causes other than vaccination.
In 2021, South Korea researchers reported that after examining the death of a 22-year-old man who died five days after receiving the Pfizer vaccine, they determined the primary cause was “myocarditis, causally-associated” with the vaccine.
In January, New Zealand researchers reported that the Pfizer vaccine was probably responsible for sudden myocarditis that led to the death of a 57-year-old woman, writing that “other causes have been discounted with reasonable certainty”.
In February, researchers in several U.S. states reported that two teenage boys who died shortly after receiving Pfizer’s vaccine experienced heart inflammation and that the inflammation was the primary cause of death.
In May, CDC researchers reported that a young boy died after experiencing post-vaccination heart inflammation, with myocarditis being pegged as the cause of death.
In September, a German researcher reported that a 55-year-old who died four months after receiving the Pfizer vaccine died of myocarditis and said “these findings indicate that myocarditis, as well as thrombo-embolic events following injection of spike-inducing gene-based vaccines, are causally associated with a[n] injurious immunological response to the encoded agent.”
And just recently, Japanese researchers reported on results from a 27-year-old man who died 28 days after admission following vaccination.
In addition, a German case report of an autopsy conducted on a 76-year-old man who died three weeks after receiving his third COVID-19 vaccination found the presence of spike protein but not the nucleocapsid protein in the deceased man’s brain and heart, proving that the vaccine (which unlike the virus only produces the spike protein) was the cause of the deadly inflammation.
More recently, a report on a series of German autopsies found the vaccine was likely responsible for three deaths from myocarditis and possibly responsible for two others. A further 20 deaths from cardiovascular causes were not determined one way or the other.
Many countries around the world are reporting high excess deaths during 2022 from mainly cardiovascular and unknown causes which remain unexplained. In Ireland, leading politician Peadar Tóibín has called for an investigation into excess deaths after they hit 17% over the summer.
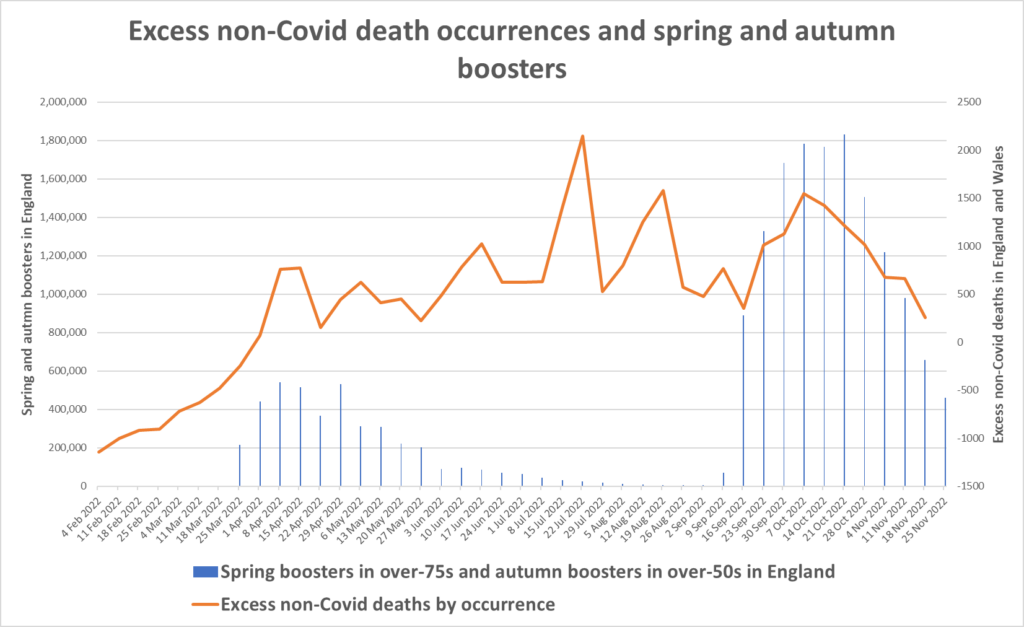
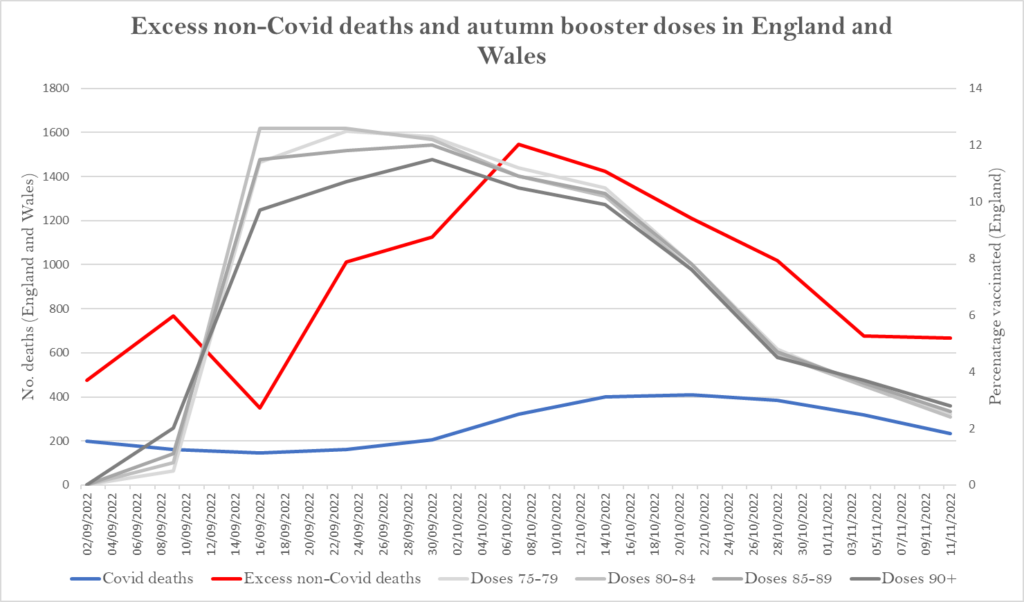
The latest data from England and Wales show that there have now been 25,918 excess non-Covid deaths since April. In the week ending November 25th, the most recent week for which figures are available, there were 11,483 deaths, which is 778 or 7.3% above the five-year average, according to figures from the ONS. Of these, 215 are due to Covid (as underlying cause) leaving 563 from an underlying cause other than COVID-19. A possible link with the vaccine booster campaigns may be observed in the charts below, which show booster vaccinations and deaths by date of occurrence.
As the weight of evidence that the vaccines can kill, suddenly and silently – even weeks and months after administration – accumulates, the blanket denials that they are playing any role in the global trend of excess deaths ring increasingly hollow. The need for a proper investigation remains as urgent as ever.