

The fifth COVID booster shot became available this week. The Federal Government recommends that all adults aged 65 and older, and all adults aged 18 to 64 at risk of severe COVID-19, or who have disability with significant or complex health needs, should get the vaccine dose. All adults aged 18 to 64 without risk factors, and at-risk children and adolescents aged 5 to 17 should consider the jab, the government suggests.
“An additional COVID-19 booster dose is anticipated to address waning of protection against severe COVID-19 prior to winter,” the Australian Technical Advisory Group on Immunisation (ATAGI) states. “This will provide an increase in protection against severe illness and protect the healthcare system during a time of high demand.”
But some doctors are sceptical of the COVID-19 vaccine, and urge caution.
Among them is Dr Christopher Neil, cardiologist and lecturer at the University of Melbourne, and president of the Australian Medical Professionals’ Society (AMPS), a group of doctors who want to provide an alternate voice to the Australian Medical Association (AMA).
“There has to be an acknowledgement that this recommendation has been made despite unprecedented signals of harm and a stifling of debate,” Dr Neil said.
He was in Canberra earlier this month to host an event discussing Australia’s COVID-19 response, meet federal politicians – including Senators Ralph Babet (United Australia Party), Gerard Rennick (Liberal National Party of Queensland), and Malcolm Roberts (One Nation) – and call for an end to medical censorship and vaccine mandates. (Victoria and Queensland require healthcare workers to be up to date with their COVID vaccinations.)
Dr Neil points to the report published last August by Dr Phillip M. Altman, a clinical trial and pharmaceutical regulatory affairs consultant. The report – endorsed by Professor Wendy Hoy, Director of the Centre for Chronic Disease, University of Queensland – argues that COVID-19 vaccines are not really vaccines, but experimental gene-based therapies, and have been associated worldwide “with far more deaths, illnesses, injuries, and disabilities than any other therapeutic agent in the history of medicine”.
According to Dr Altman, the vaccines use technology never deployed in a fully approved therapeutic product, and only investigated in relatively early clinical research for certain cancers and rare genetic disorders. They were only provisionally approved, not fully approved, by the Australian drug regulator, the Therapeutic Goods Administration (TGA). They do not prevent SARS-CoV-2 infection or transmission of the virus, and any immunological protection wanes rapidly. Side-effects of the vaccine include heart attack and strokes; cancer; infertility and miscarriages; and myocarditis, pericarditis, and death in children. Dr Altman believes that, “in light of the known unprecedented level of serious adverse reactions and death attributed to their use”, the use of vaccines must be reconsidered.
The AMPS agrees.
“We believe this debate has to be had urgently,” Dr Neil said. “If Dr Altman’s suspicions are correct, recommendations for further dosing could be detrimental to the community.”
TGA rejects Altman report
The TGA, however, rejected Dr Altman’s report, stating that it contained “many remarkable scientific errors of fact and significant misinterpretations” about the safety of COVID-19 vaccines; it was self-published without peer review, so was not credible and had not been through the scrutiny required for publication in a reputable scientific journal.
“The mRNA vaccine platform is not gene therapy,” the TGA said. “It is remarkable that people who have worked in universities are not aware of this basic fact. mRNA vaccines have also been subject to research for decades. It was first tested in the 1990s, including in the contexts of Zika, rabies, and influenza vaccines, not just certain cancers and rare genetic disorders as alleged in the report.”
The TGA dismissed claims there were more reported injuries from the COVID-19 vaccines than for all other medicines and vaccines as false and unscientific.
“There is no credible evidence to suggest that COVID-19 vaccines cause heart attacks, strokes, cancer, infertility, or miscarriages,” the TGA said. “These conditions have not been linked to COVID-19 vaccination in Australia or internationally from data from the billions given internationally.” Deaths in children linked to COVID-19 vaccines was misinformation.
Dr Neil: Unprecedented adverse events from vaccines
According to the National Centre for Immunisation Research and Surveillance (NCIRS), more than 6.8 million people around the world had died from COVID-19 as of 10 February. In Australia, 18,828 people had died, and 11.3 million people were infected.
But in Dr Neil’s view, Australia is experiencing a highly significant iatrogenic event – that is, medical examination or treatment (specifically the vaccines) that causes illness.
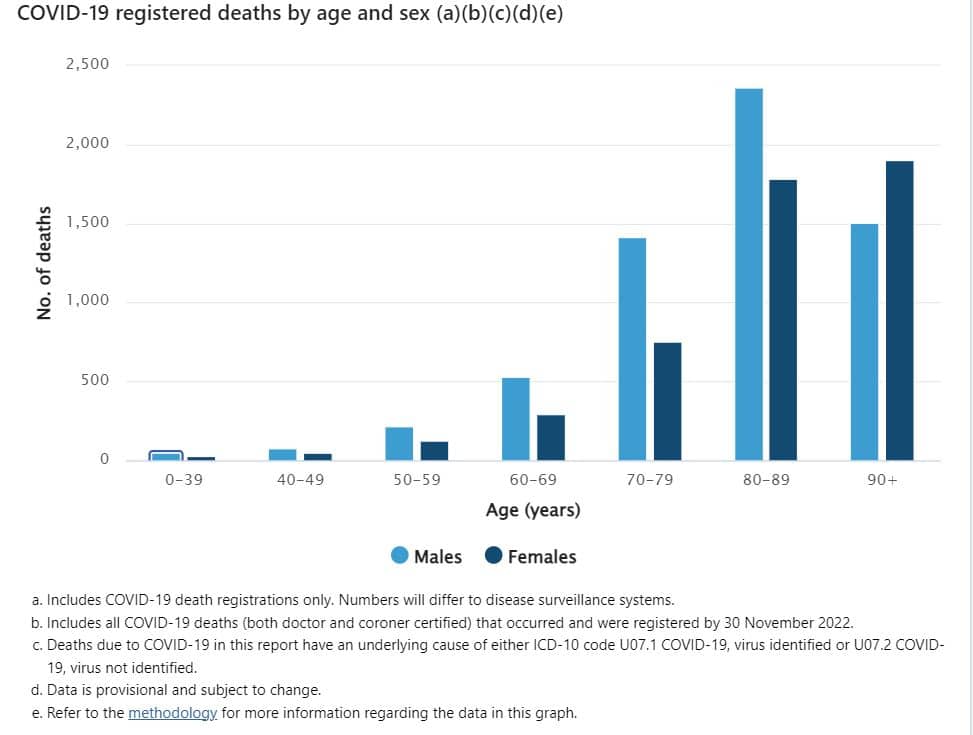
Serious illness and death attributed to COVID, Dr Neil argues, are heavily weighted to the elderly and those with known comorbidities, while younger Australians are relatively resistant to the virus. The Australian Bureau of Statistics recorded that 13,641 people died with or from COVID-19 by 30 November 2022; COVID-19 was the underlying cause in 81.2 per cent (11,077); the median age for those who died from COVID-19 was 85.4 years, and 80.1 per cent had pre-existing chronic conditions.
Conversely, Dr Neil states, the vaccines’ adverse effects are unprecedented: more than 3 million reports and nearly 62,500 deaths worldwide up to June 2022. (Dr Neil estimates the real figures might be 10 times higher.)COVID-19 injectablesAdverse event reportsDeathsEuropean Medicines Agency1,845,71945,982US VAERS835,06213,388Australia TGA132,155889UK Yellow Card458,4632,191TOTAL3,270,85962,450
In Australia, he remarks, the TGA received more adverse event reports between 2021 and June 2022 for the COVID-19 vaccines than for all other vaccines in the past 50 years. This table he drew up last year, based on the TGA’s Database of Adverse Event Notifications:Non-COVID vaccines (1971–2021)COVID-19 injectables (1 February 2021 – 8 June 2022)Number of adverse event reports19,330132,668Number of reaction types1,4923,660Number of adverse reactions non-COVID vaccines43,878433,669Number of adverse reactions per adverse event report2.273.27
Those figures, Dr Neil said, do not match any previous rollout. The argument that there are more adverse effects because the COVID rollout is bigger cannot be made, he says; the flu vaccine, for instance, has been used on a comparative scale.
“But that one is tried and true, acceptable to the community. Because of long-term experience and good manufacturing practice, problems have been ironed out over time.”
The visibility of vaccine-injured people is growing, Dr Neil said; and the exact numbers of people living with chronic impairment are not known.
Professor Kerryn Phelps AM, former president of the AMA, is also concerned. In a submission to a Federal Inquiry into Long COVID and Repeated COVID Infections, she stated that she had suffered a vaccine injury from her second dose, while her wife had a severe neurological reaction to Pfizer. Her wife’s “devastating effects” – burning face and gums, damaged nerves, numb hands and feet – continue 18 months later, now with fatigue, nerve pains, altered sense of smell, visual disturbance, and musculoskeletal inflammation. Many doctors, patients, and others in the community have experienced serious and persistent adverse events, including cardiological, rheumatological, and autoimmune reactions, and neurological consequences, Dr Phelps wrote.
She called for more research on immunisation side effects; streamlining the reporting process for adverse events; identifying barriers to reporting adverse vaccine reactions and streamlining processes; follow-up of adverse COVID vaccine events reported in TGA; information packages for GPs and medical specialists on vaccine adverse events; and research into underlying mechanisms of vaccine injury, and treatments for vaccine injury.
TGA: Adverse events are not necessarily related to vaccination
The TGA states that COVID-19 (like all medicines) may cause some side effects – most often injection-site reactions (sore arms) and more general symptoms (headaches, muscle pain, fever, chills). Reporting rates of adverse events are stable – at 2.1 per 1,000 doses (0.2 per cent). However, according to AusVaxSafety (part of the NCIRS), 44.1 per cent of people surveyed reported at least one adverse event from vaccines. It notes: “Adverse events are self-reported, have not been clinically verified, and do not necessarily have a causal relationship with the vaccine.”
The TGA attributed the high number of suspected adverse event reports to intense public interest in the vaccines, the high level of awareness during the pandemic, and the TGA and Government’s promotion and facilitation of adverse event reporting.
“Adverse events are reported on the basis of suspicions, and anyone can make a report,” the TGA said. “The adverse event could be a coincidence, due to underlying illness or other factors. With rapid whole population vaccination, it is possible that some people will develop new unrelated symptoms or illnesses within days or weeks following vaccination. However, it is false to automatically conclude they were caused by the vaccine.”
The TGA is monitoring and reviewing reports of myocarditis and pericarditis (inflammation of the heart or membrane around the heart). It states that these are temporary conditions, and most people get better after a few days. Myocarditis is reported in one to two in every 100,000 people who receive Pfizer and in two people in every 100,000 who receive Moderna. The TGA stated that myocarditis and pericarditis were seen in the general population from a variety of causes, including after COVID-19 itself, and not all cases that occur after vaccination were necessarily caused by the vaccine. Several studies showed that the rare cases of myocarditis after COVID-19 vaccination are milder than myocarditis after coronavirus infection.
The TGA’s COVID-19 vaccine safety report includes regular updates regarding myocarditis and pericarditis reporting rates.
Dr Neil: Vaccines were undertested
Dr Neil believes that vaccines were rushed out before being properly tested.
“Australians were assured that, although these vaccines were developed quickly, they were safe and effective, and the safety monitoring would be very robust and presumably responsive,” he said.
But, he argued last year, the rush to market and provisional approval occurred despite the absence of the usual pre-clinical studies, including testing for carcinogenicity and genotoxicity. For instance, a peer-reviewed investigation demonstrated that mRNA-derived spike proteins enter the cell nucleus and interfere with DNA.
Dr Neil believes the TGA’s Provisional Approval Pathway facilitated the rapid entry of significantly undertested products into the Australian market, despite their being highly novel and experimental. The TGA states that the Pathway “provides access to certain promising new medicines where we assess that the benefit of early availability of the medicine outweighs the risk inherent in the fact that additional data are still required”. But, Dr Neil said, this allowed drugs with less of a track record, safety data, or preclinical and clinical studies to guarantee safety and efficacy.
“You can’t have a provisional approval system that accelerates the process and allows a compromise with safety without a corresponding beefing-up of the whole deal of drug safety monitoring,” Dr Neil said. “If you leave that to be a broken system, and change the criteria from the traditional, decades-old standards of safety rigour, you’re going to have human casualties – and that has been the case.”
The AMPS, Dr Neil said, can document major flaws at multiple levels with drug safety monitoring in Australia.
“It’s not the first time that questions have been raised about how well we monitor and how responsive our monitoring system is,” Dr Neil said.
In 2010, the Western Australian Department of Health suspended its influenza vaccination program for children, following reports of severe side-effects. The Stokes Review found that the state and the Commonwealth were slow to respond to apparent emerging adverse events arising from the 2010 vaccination program. (The TGA, however, responded that the Stokes Review “contains significant errors, misinterpretations and flawed conclusions”.)
TGA: Full and thorough assessment
The TGA, however, stated that it fully and thoroughly assessed the Cominarty (Pfizer), Spikevax (Moderna), Nuvaxovid (Novavax), and Vaxzevria (AstraZeneca) vaccines, and all are safe and effective at preventing severe illness, hospitalisation, and death from COVID-19.
The TGA provisionally approved the vaccines after a complete assessment of all available data – the same process as any vaccine approved in Australia. No part of the process was rushed, and no emergency authorisation was granted.
The TGA said that it established the acceptable safety, quality, and efficacy of the vaccine based on a comprehensive evaluation by clinical and scientific experts of clinical studies, non-clinical and toxicological studies, chemistry, risk management, and manufacturing information. It sought advice from the Advisory Committee on Vaccines, an independent clinical expert committee.
“A vaccine is only provisionally approved by the TGA if this rigorous process is completed and the benefits of the vaccine are considered to be much greater than any potential risks,” the TGA said.
The TGA said that while it might seem vaccines were developed quickly, collaboration between researchers, scientists, manufacturers, and distributors around the world, unprecedented funding, and faster technology sped up the development of the vaccines. Data from previous coronaviruses (severe acute respiratory syndrome / SARS in 2002, Middle East respiratory syndrome / MERS in 2012) gave researchers a head start in developing the vaccines.
Many leading scientific journals published peer reviewed articles that confirm the efficacy of the provisionally approved COVID-19 vaccines, the TGA stated. A Danish cohort study, for instance, showed that three vaccine doses substantially increased the level and duration of protection against infection with the Omicron variant and provided a high level of sustained protection against COVID-19 hospitalization among the people over 60. The New England Journal of Medicine, the Centers for Disease Control and Prevention, and The Lancet found that bivalent mRNA boosters were more effective against severe omicron infection than monovalent boosters.
“The safety and efficacy of the COVID-19 vaccines has been thoroughly substantiated by real-world use in hundreds of millions of people worldwide, demonstrating that vaccination is highly effective at preventing serious outcomes from COVID-19 including hospitalisation and death,” the TGA said.
The NCIRS states that the mRNA (spike protein) in some COVID-19 vaccines like Pfizer and Moderna is not harmful; it gets broken down and removed very quickly from the body. The only confirmed serious side effect is anaphylaxis, which can occur after any vaccine or medicine, and is treatable. Anaphylaxis is rare: as of December 2020, there were 11 cases per million people for Pfizer, and 2.5 cases per million people for Moderna.
AMPS: Doctors cannot question vaccines
“Medical censorship compounds the problem,” Dr Neil said. He believes that government ‘gag orders’ prevent doctors from speaking out about vaccines, and that doctors cannot question science underlying COVID vaccines, or government messaging encouraging Australians to be vaccinated.
In March 2021, the Australian Health Practitioner Regulation Agency (APHRA) warned: “There is no place for anti-vaccination messages in professional health practice, and any promotion of anti-vaccination claims, including on social media and advertising, may be subject to regulatory action.”
In Dr Neil’s opinion, this unilateral action compromised proper and informed consent in Australia: it inserted APHRA and the National Boards between clinicians and patients, while health professionals were mandated to support the government campaign to have the Australian population injected with drugs for which there was no adequate safety or efficacy data.
“We effectively could not speak negatively about the vaccinations that were being rolled out, because we could not, in their view, undermine the government rollout plans,” Dr Neil said.
“The voice of doctors and nurses is compromised; the voice of genuine clinical experts is muzzled by the gag order. If it wasn’t, we could have spoken against mandates more articulately, and had a more robust debate in the community, and brought to light more of the valid points that required logical consideration.”
In his view, this conflicts with the doctors’ code of conduct, which requires the medical profession to make the care of patients their first concern, and not be influenced by big pharmaceutical and other medical marketing.
“APHRA has never once acknowledged we have a duty of care for the community and our patients, if we feel their safety is in question,” Dr Neil said.
“We have to be able to speak out – to blow a whistle – to call time out on a pharmaceutical or a hazardous product in the community.
“Doctors still don’t feel safe or able to fully express their concerns, either in advising their patients or in the public square. Many are still holding out in denial.”
Dr Kerryn Phelps also informed the federal inquiry that few in the medical profession wanted to talk about vaccine injury, and her attempts to discuss the issue were met with obstructions and resistance.
“Regulations of the medical profession have censored public discussion about adverse events following immunisation, with threats to doctors not to make any public statements about anything that ‘might undermine the government’s rollout’ or risk suspension or loss of their regulations,” she wrote.
Some doctors have been suspended without income after regulators were told they issued vaccine exemptions to patients; others received notice they are being investigated. Every doctor knows of these cases, Dr Neil said.
“That has a chill effect. Doctors are not renegades. They’re very circumspect, they’re used to thinking about what they do, whether it conforms to the peer group. They don’t want to be the only ones doing something, because that’s one way they stay within a zone of good practice and safety. In this case, that’s been inverted.
“The aspect of being in keeping with the practice of their peers, as influenced by the government, is keeping them from responding to an iatrogenic crisis from these shots,” Dr Neil said.