
But the injections caused an iatrogenic pandemic in 2021/2022
There Never Was A Covid Pandemic In 2020
This new analysis of raw, official, unmanipulated data from The Australian Bureau of Statistics (ABS) confirms what many of us, who trust our own eyes and ears, have been suspecting for years: There never was a Covid pandemic in 2020. Let’s be clear: There was a virus that was making people sick and killing some people, but not more so than in any previous years. The author makes a good case that the narrative of Covid virus pandemic was based on unsuitable PCR tests. The author, Wilson Sy, uses the Bradford Hill analysis in his 25-page long paper, titled: Australian COVID-19 pandemic: A Bradford Hill analysis of iatrogenic excess mortality Wilson Sy is an analyst with 62 publications.
And there is more: The author argues convincingly that the actual Covid injections caused an iatrogenic pandemic in Australia in 2021 and 2022. Iatrogenic means caused by medical examination or treatment. If this work holds up to scrutiny, it looks like this is convincing evidence that the state of Australia is directly responsible for the deaths of tens of thousands of its citizens by manipulating, coercing, or mandating them to take unsafe, deadly Covid injections. This is another confirmation of whatSteve Kirsch has been saying for a long time now.
It is not based on opinions, speculations, modeling, or propaganda. Instead, it is based on official raw data of events that actually happened in Australia. Data doesn’t lie.
Methodology: Bradford Hill Analysis Of Excess Mortality
Further, it uses a simple, but robust methodology widely accepted and used in science to prove causality: The Bradford Hill analysis.
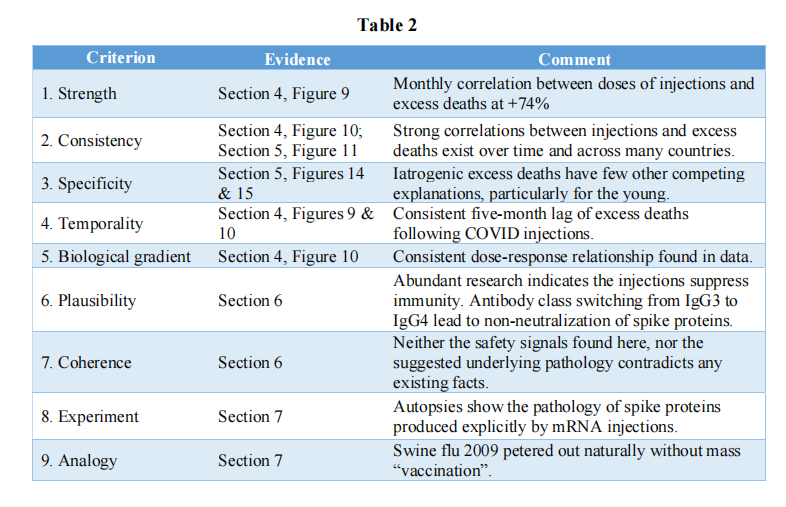
The Bradford Hill criteria include nine viewpoints by which to evaluate human epidemiologic evidence to determine if causation can be deduced: strength, consistency, specificity, temporality, biological gradient, plausibility, coherence, experiment, and analogy. Quote Source
It uncovers lies, disinformation, and misrepresentations by the government and mainstream media. This caused many people to die. And many more people will die if this analysis is not taken seriously and repeated in many more countries. The author concluded:
This study has introduced a […] methodology, which should be used by other countries, […], to replicate and investigate the likely iatrogenic origins of their own pandemics. Billions of lives in the world are at stake from the potential findings of the research.
Table 2 provides a summary of how the nine criteria were applied
No “Covid Pandemic” in 2020
Australian official mortality data show no clear evidence of significant excess deaths in 2020, implying from an older WHO definition that there was no COVID-19 pandemic.
WHO changed the pandemic’s old definition, making it much easier to declare one. For a detailed discussion see here
Seasonality analysis suggests that COVID-19 deaths in 2020 were likely misclassifications of influenza and pneumonia deaths.
You might remember reports that in 2020 there was almost no influenza and pneumonia. Some voices suggested this was because of more handwashing and lockdowns. According to the author, all so-called Covid cases were “diagnosed” with the PCR test which never was a diagnostic tool to start with. People who pointed that out in 2020 were labeled “conspiracy theorists”, vilified, and censored. Here is the data:
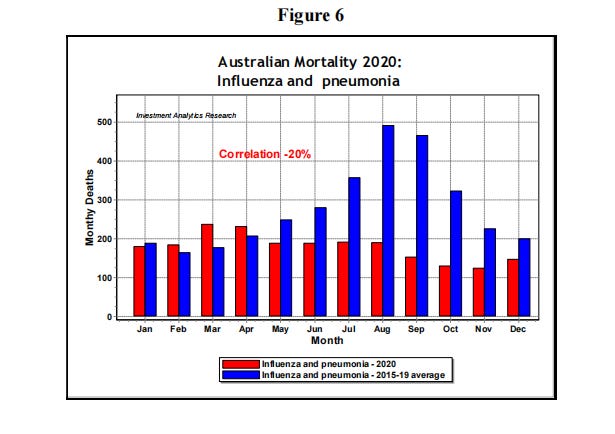
By comparison, 2020 was a very odd year, when deaths from influenza and pneumonia (red bars in Figure 6) substantially disappeared for several months around their normal peaks in late winter. The correlation between normal fluctuations and 2020 fluctuations was negative, at -20%, indicating a significant seasonal anomaly.
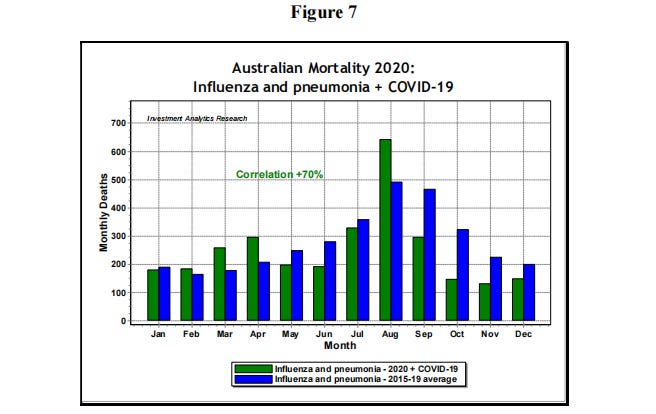
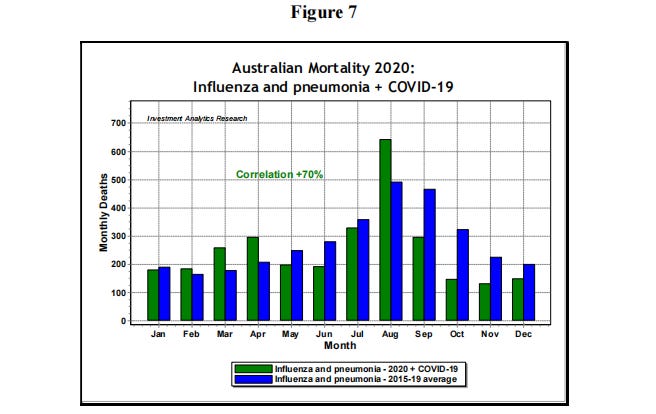
However, COVID-19 is a respiratory disease, with similar symptoms to influenza and pneumonia (I&P) and there were surges in COVID deaths around August in 2020, particularly in Victoria. If the deaths of I&P and COVID-19 are added together, then the comparison to normally expected seasonality is shown in Figure 7.
The author concludes:
In the I&P comparison in Figure 7, the green bars including COVID deaths are now consistent with the blue bars representing the expected seasonality pattern of previous years, with a positive correlation of +70%. In view of the poorly defined characteristics of COVID-19 infection and the subjective attribution of COVID-19 deaths as discussed in the introduction, there is a strong possibility that COVID deaths may have been substantially misclassified I&P deaths.
In other words, the only criteria to call an infection “Covid” came from unfit PCR tests. In reality, most of these infections were actually normal annual influenza and pneumonia, mislabelled as “Covid”.
No “Covid” pandemic in 2020, but a Covid Injection Pandemic from 2021 to 2023
Australian excess mortality became significant only in 2021 when the level was high enough to justify calling a pandemic. Significant excess mortality was strongly correlated (+74%) with COVID-19 mass injections five months earlier. Strength of correlation, consistency, specificity, temporality and dose-response relationship are foremost Bradford Hill criteria which are satisfied by the data to suggest the iatrogenesis of the Australian pandemic, where excess deaths were largely caused by COVID-19 injections.
They say that pictures say more than a thousand words. Here are two:
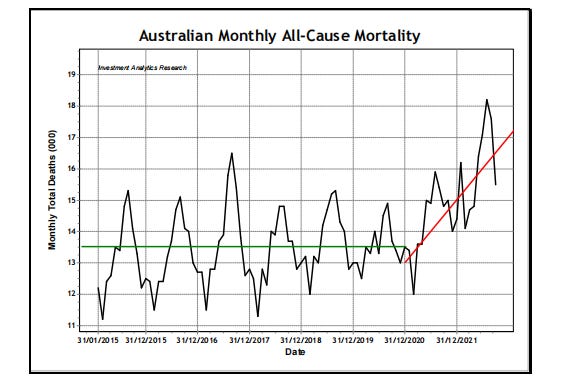
This is the last seven years. Each segment on the x-axis represents a year. The last segment before the red line represents the year 2020. Excess death is seasonal – more people die in winter. This explains the peaks in each year. 2020 had actually fewer excess deaths than the previous five years, ergo no pandemic in 2020. The red line shows the sharp rise of excess death after the Covid injections roll-out. This rise in excess death shows an injection-induced pandemic in 2021 and 2022.
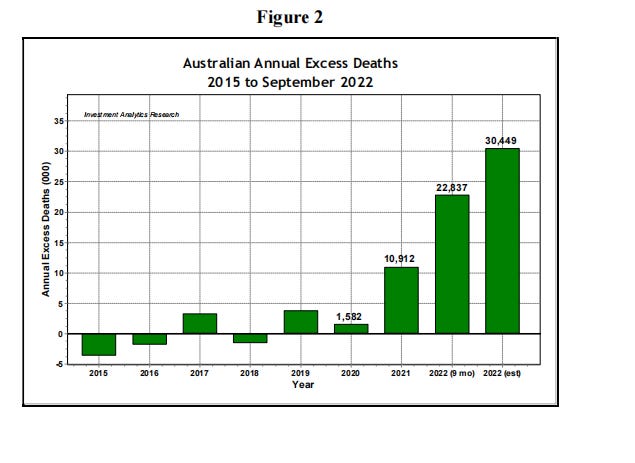
The excess deaths were only 1582, in line with previous years. Some would argue this is because of the harsh measures of masks, closed borders, and lockdowns. Others would argue that those measures actually prevented herd immunity and that’s why the Covid virus (or was it actually influenza or pneumonia?) is still around. The analogy with the swine flu below seems to support the latter.
In 2020 there was a pandemic preparedness plan which recommended against lockdowns, masks, and travel restrictions, advocating for open boundaries but protecting vulnerable people. The logic was clear. Let the virus spread as fast as possible amongst young and healthy people to reach global herd immunity. A proven success story throughout evolution.
But this time other forces intervened. The exaggerated wrong modeling of the Imperial College London caused panic and fears of overloading our hospitals. Bill Gates is a big donor to the College. All preparedness plans, the thoughtful work of generations of scientists, were abandoned overnight. The rest is history.
After a year of brutal lockdowns and other restrictions, supported by military-grade psych-op 5th generation warfare against their own people (see Robert W Malone MD, MS and Maajid Nawaz for detailed evidence), the new mRNA vaccines were about the only state-sanctioned answers to the blown-out-of-proportion threat of a Covid virus.
From March 2021 until September 2022, a 2 1/2-year period, over 60 million doses of an unknown substance with very little efficiency and safety data, were injected into over 20 million Australians’ arms. Following that, about 60.000 more people died than expected. That is approx. 2000 per month or an average of 24.000 per year. This is more than 20 times the annual road toll. Australia lost 34,000 service personnel during World War II. (Source) The jabs doubled that.
But is this proof that the Covid injections largely caused that? What about all the other possible reasons for so many extra people dying? This mainstream article, titled “Why are more people dying in Australia? Many questions remain”, was suggested by Google on the first page of my search: “what causes the excess mortality worldwide”.
It was a painful read. They first did downgrade the official ABS rate of 16.6% to 12%. Then, so-called experts wildly speculated, without providing much evidence at all. From insufficient exercise to overloaded hospitals and anything in between.
However, what really stands out in this article is what is not talked about at all: The Covid injections. If you want to teach a student the meaning of the metaphor “Elephant in the room”, this would be the perfect resource. The fact that more and more people started dying pretty much after more than 20 million Australians were injected was ignored.
This obvious outrageous omission of the most probable cause points only to one thing: The people in mainstream media are still trying to protect and uphold the biggest fraud and lie in history: That these injections are safe and effective. And with that, they commit mass murder. As astounding as it may sound to us alternative news readers, many people in Australia still believe and trust the mainstream media. The irony is, that MSM is killing off its own readers.
So how does Wilson Sy further prooves that this excess mass dying is caused by the injections? He already showed a 74% correlation between injection and death. This is the strength criteria. Regarding the “Consistency criteria” over time he offers Figure 10 below, Total Doses vs Excess death adjusted by 5 months lead time.
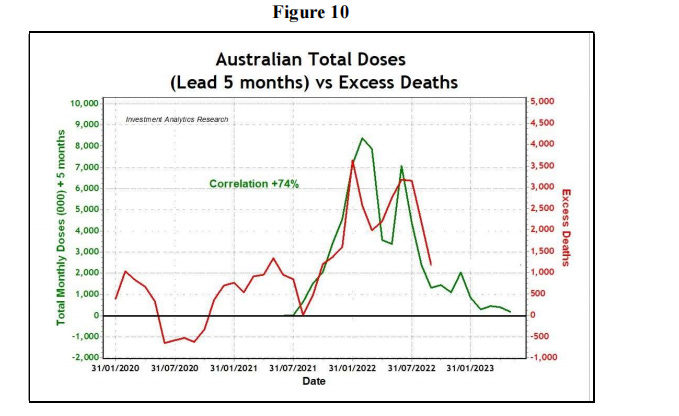
The correlation is all there to see. He also calculates a 31% correlation when comparing other countries. It happens all over the world.
Specificity
Another useful criterion of Bradford Hill causality is “specificity”, which is related to the question of whether there are competing causes for the excess deaths, with similar strengths of association.
Sy has done a good job to proof correlation and consistency so far. But correlation, even if consistent over time and in other countries, doesn’t prove causation of mainly one cause: The injections. He is doing this by looking at a specific subgroup: The youngest age group. Here is why:
The specificity of COVID injections on excess mortality is much clearer for the young than the old, due to fewer possible confounding factors. In 2019, the Australian residential population was 25.35 million, of which 15.17 million were in the 0-44 age group, or about 60% of the total population. Despite the smaller number of excess deaths for the youngest 0-44 age group, the statistical signal is dramatic, because the group normally have a very low mortality risk.
In lay terms, old people die of many causes. Young people hardly die at all and of very few causes. They also very rarely die from Covid itself which puts to bed the speculation of Covid as a reason for excess mortality for this group, in my opinion.
What is highly statistically significant is the youngest 0-44 group, with their excess mortality in 2022 was about 160% above historical expectation compared to normally less than 20% fluctuations for all age groups before 2022. Whilst the youngest group has excess deaths at “only” 400 per month in 2022, their expected mortality is normally very low. Therefore, proportionately, the harm suffered by the youngest age group has been very high
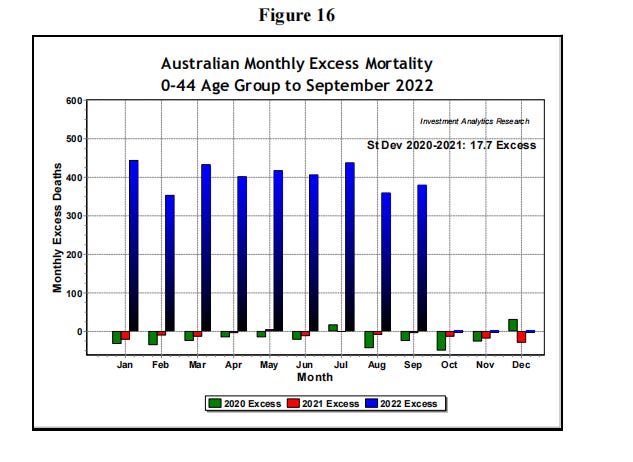
The excess deaths for this age group was consistently around 400 per month in 2022, which means 23-sigma events were occurring for every month in 2022. This represents metaphorically a 9.5 earthquake on the Richter scale for epidemiology.
Apart from mass COVID injections which were often administered coercively, what other causes, satisfying basic Bradford Hill criteria, could possibly explain this enormous surge in excess deaths among the young?
Coherence and Plausability
Is this thesis coherent with other research or are there findings that strongly contradict it? Is there research that supports and offers explanations of what has happened? The author thinks so:
On Bradford Hill’s coherence and plausibility, the suggestion of iatrogenic origin of excess deaths following five months after COVID injections does not contradict any research on “vaccine safety”. The clinical trials conducted were much shorter than five months.
That is, the Pfizer trial data analyzed were conducted over eleven weeks or 77 days, about half of the time necessary for fatalities to occur per the above empirical findings, so the suggested iatrogenesis is coherent and not in conflict with any known facts.
Are there any plausible biological mechanisms which could explain the causal impact of COVID-19 injections on the excess mortality of the young and healthy? In the past three years, there has been a deluge of research published on how the spike protein, either from the assumed SARS-CoV-2 virus infection or generated from the mRNA injections, could lead to inflammation in various organs causing death.
In a recently published clinical study [19] of the mRNA injections, production of neutralizing IgG3 antibodies against the spike protein was observed to switch over time to the production of non-neutralizing IgG4 antibodies. Thus, the class switching may reduce the rate of clearance of the toxic spike protein which may accumulate sufficient titers to cause pathogenesis and mortality.
The five-month lag between injections and mortality found in this paper may be related to the switching time between the classes of antibodies, which was not the focus of the cited clinical study, but it provides some useful indications.
Experiment and Analogy
To start with, the author points out that medical experiments were discouraged in Australia to prevent “vaccine hesitancy.” Also, post-mortems and autopsies were not encouraged.
Australian governments have deliberately discouraged such “experiments” because they may lead to findings which cause “vaccine hesitancy”. For example, Australian doctors have been threatened with up to $20,000 for using serological tests to verify the results of the PCR tests for COVID-19 diagnosis [22]. Nevertheless, the scientific imperative is strong enough to have led to several post-mortem studies to discover the “smoking gun” evidence of spike proteins from COVID injections.
What follows is a detailed, very specific discussion of the spike protein attributes and behavior and related research which is too complex for this small mind to be summarized coherently. So I have to refer you to the original text.
As an example of analogy, he refers to the swine flu pandemic:
An analogy to the current COVID-19 pandemic is the 2009 “Swine flu” pandemic due to the H1N1 influenza virus. Then, as now, the pandemic was called, based not on fact, but on expectations of a highly infectious and very deadly disease projected by the Oxford computer models. The main difference is that the 2009 “pandemic” was never allowed to be transformed to an iatrogenic pandemic and it quickly died out on its own accord, amounting ultimately to a weaker form of the seasonal influenza. The episode had more cases worldwide, but fewer deaths (about 18,000) and a much lower case fatality rate than the seasonal flu [28]. On an excess mortality definition, the 2009 “Swine flu” season was not a pandemic.
Conclusion
Based on mortality data, the Australian COVID-19 pandemic did not begin until the advent of mass mRNA injections in 2021. It is ironic that mass injections which were introduced to mitigate a non-existent pandemic created a real iatrogenic pandemic. This study, backed by a Bradford Hill analysis, has shown that more injections administered to reduce the pandemic, had the opposite effect of causing more excess deaths to increase in the pandemic.
The very large excess deaths observed from the data imply that the mortality risk/benefit ratio from COVID injections is very high. That is, the harm or risk realized has far outweighed any benefit from COVID injections.
Source – https://markusmutscheller.substack.com/p/hard-raw-data-there-never-was-a-covid