
Pandemic response a failure, preeminent cardiologist says

On June 29, 2022, Dr. Peter McCullough, M.D., testified to the Texas Senate Health and Human Services Committee about what we have learned during the COVID-19 pandemic. He called his 17-minute presentation “Pandemic Lessons Learned.”
Who is Peter McCullough, M.D.?
Peter McCullough is one of the country’s best published and most respected cardiologists. He has practiced conventional cardiology throughout his successful career and never had a reason to question medical authority or vaccine safety. All of that changed during COVID. As he explained to the same committee in March of 2021 (you can find a transcript of that testimony on my website), McCullough was deeply disturbed that the medical establishment insisted COVID wasn’t treatable.
You can read the full transcript of his testimony below. But for anyone who wants the cheat sheet…
The Most Important Take-aways:
1. COVID-19 is treatable. Early treatment reduces your risk of hospitalization and death by 95 percent, according to Dr. McCullough.
2. Remdesivir is not a safe or effective drug and should not be used to treat COVID-19
3. Vaccines against COVID-19 were not adequately studied before being made available to the public.
4. COVID-19 vaccine program should be immediately halted worldwide.
5. Doctors, nurses, and patients who share their stories should not be censored or vilified. We need to pay attention to their experiences, not seek to silence them.
Pandemic Lessons Learned
Dr. Peter McCullough: Madam chairman, ladies and gentlemen: I am probably well known to the committee, I testified here on March 10th, 2021. I’m a practicing internist and cardiologist in Dallas, Texas, and I’m an expert on COVID-19.
I have 56 peer-reviewed publications on the pandemic. Particularly, on how to treat the infection, and over 770 overall publications in the National Library of Medicine, and well over a thousand overall medical communications.
I’ve served on two dozen data-safety monitoring boards for large pharmaceutical and device and in vitro diagnostic studies; and I consider myself both an expert on the COVID-19 virus as well as on drug and device and biological agents safety.
Here are my comments.
A Duty to Treat the Patient
There has always been a duty to treat COVID-19. It started with the very first case—as soon as we recognized that this was a potentially fatal infection.
When a patient could have died of this infection, at that moment, and we understood it early based on risk stratification (based on age, medical problems, and severity of symptoms upon presentation), there was a duty to treat that patient. Period.
If a doctor did not treat that patient when a patient sought help, there was a duty to refer. From the very beginning, there was a community standard of care—though from the very beginning, it evolves over time. In many situations like this or with rare diseases, the community standard of care may be one doctor in that community who’s going to take on the challenge of treating that patient—but that becomes the community standard of care.
Early, there was use of a variety of drugs that became standard of care, as evidenced by surges in use of these drugs, and they included hydroxychloroquine, ivermectin, prednisone, and budesonide. There were giant surges and use of these drugs as evidence that these were outpatient evolving standards of care.
Now there is surge of use in Paxlovid and a minor surge in Molnupiravir.
There has always been a community standard of care for early treatment.
Lessons learned for this committee. There have been eight hours of testimony today. [But] not a single presenter could tell you what patients in these data sets received early treatment and what was their outcomes. Not a single presenter knew who had received early treatment and what was the degree of complexity of that early treatment.
Next Time We Must Convene an Early Treatment Committee
Lesson learned. Next pandemic immediately get an outpatient early treatment committee together. Their objective is to reduce the risk of hospitalization and death. That is the overall objective of this pandemic: Keep people out of the hospital and keep them alive. If they can get through this illness at home, that was your mission from the very beginning on early treatment.
Fortunately, there have now been about 1,400 studies. There have been hundreds and hundreds of randomized trials. And we know that sequenced multi-drug therapy that addresses viral replication, inflammation, or cytokine storm and thrombosis is theapproach in handling this.
Dr. Procter is here. He’s published two very good studies right from the state of Texas. Dr. Vladimir Zelenko in Monroe, New York. Dr. Raoult in France.
All the data are cohesive: that the early protocols—the very early—had 85 percent reductions in the risk of hospitalization and death.
Early Treatment Reduces Risk of Death by 95 Percent
Now with monoclonal antibodies, Paxlovid, and others, I’ve testified under oath in the U.S. Senate on January 24th, 2022, based on my expert opinion there is now a 95 percent risk reduction for death and hospitalization if early treatment is provided.
Conversely, I’ve reviewed hundreds if not thousands of reports of patients who were hospitalized and died. Hundreds, if not thousands of reports. The real outcome of hospitalization and death is a product of not receiving early treatment.
Whether someone’s vaccinated or not, the vaccination is irrelevant because the vaccination is not a treatment.
What’s relevant is: Was the patient treated before the hospital? And every single case, and in every single patient outcome that I can see, the reason why they were in the hospital is they received either zero outpatient treatment or they received inadequate treatment that was received too late.
So a committee like this lesson learned: it’s always going to be about treating the next infectious disease early.
In terms of inpatient care and the overall landscape of what happened timeline, I think the charge of the committee is pay attention to big developments! Pay attention to these.
In May of 2020, there was a U.S. Senate hearing on the use of corticosteroids. Pay attention to that … You heard confusing testimony. Some of these doctors didn’t know if steroids worked or not. That was a landmark event, where it was clear that steroids worked, and it should have rapidly been instituted as a standard of care in the hospital.
Another giant development was I had published the first overall treatment protocol paper in a major medical journal, August 7th of 2020, but rapidly after that in September of 2020 there already was a home treatment guide by the Association of American Physicians and Surgeons. When there is a physician group that publishes a home treatment guide, pay attention to that.
Remember the Infectious Disease Society of America always had the first set of guidelines and then the NIH. They still to this day do not have a comprehensive outpatient treatment guideline.
That’s the reason why AAPS filled in, Frontline Critical Care Network filled in, Truth for Health Foundation, Frontline Doctors, and others. When other physician organizations based on consensus and data fill in the gaps, pay attention to that. Very very important.
Remdesivir Responsible for Kidney, Liver Injury
When an organization puts out a negative position on a drug. A negative position. This is really important and it’s a worldwide organization, you must pay attention to this.
November of 2020, the World Health Organization says stop using remdesivir. Stop it! It’s bad. It doesn’t work and it’s leading to more deaths, it leads to kidney injury and liver injury.
The immediate thing this committee should have done is [address who’s using remdesivir in the state of Texas and let’s talk about it.
Now whether or not the NIH disagrees with it or the WHO, that’s got to be vetted, but the question should have been asked. We needed to reexamine this. Were Texans going to be hurt by this drug?
The World Health Organization, European Society of Critical Care said yes [people were hurt by remdesivir]. And that went on under this committee’s watch.
These are very very important. Lesson learned. Pay attention to the big developments.
We’ve covered monoclonal antibodies well enough.
COVID-19 Vaccines Not Adequately Safety Studied
My second set of comments is about the COVID-19 vaccines. The COVID-19 vaccines went through clinical trials and had two months of observation. The standard regulatory guidance was 24 months for live attenuated, killed, or antigen-based vaccines.
These were genetic gene transfer technology vaccines. They’re classified that by the FDA, they needed five years of observation. All that was thrown out. There were no carcinogenicity studies. No mutagenicity studies. There were no teratogenicity studies.
So when they came out they were, and still are today, Emergency Use Authorized investigational. Which means the consent form says, we don’t know if these work or not, and we don’t know if they’re safe long-term. The consent form still says that.
Under your watch, vaccine mandates started happening in this state for investigationa,l experimental products.
COVID-19 Vaccines Highly Problematic
We knew by January 22nd, there was a problem.
Because the U.S. CDC Vaccine Adverse Event Reporting System had too many deaths that have already happened with a COVID-19 vaccine then they had from all the prior vaccines combined.
January 22nd of 2021, the warning bells came off and then nothing happened.
We knew on January 29th through Freedom of Information now our U.S. FDA, Center for Disease Control, were supposed to be putting out monthly safety reports for America–-No safety report.
Lesson learned for this committee: Get a vaccine safety committee together. Get them together and start having them meet.
If you’re not seeing safety being provided at a federal level. Remember safety safety safety. It would have been wonderful if these vaccines would have worked. But it was all about safety.
We now know through court-ordered documents—Freedom of Information documents— Pfizer knew about 1,223 deaths within 90 days of release of their vaccine.
Pfizer knew about it.
We don’t know if the FDA knew about it.
Nobody did anything and the freight train continued.
Deaths From COVID-19 Vaccines
Now fast-forward as death started to occur, people started to get very very uncomfortable, and you saw all the push-backs, protests of all kinds worldwide, feelings of great vaccine hesitancy cause people were dying shortly after the vaccine.
Papers were published. Fifty percent of the deaths occurred within forty-eight hours, eighty percent within a week.
We know the vaccines installed the genetic material for the Wuhan’s spike protein that was manipulated in a past security lab in Wuhan, China.
COVID-19 Vaccines Cause Blood Clots, Heart Damage, Neurological Damage
There are now a thousand papers published on the spike protein and the vaccines. A thousand that deal with vaccine injuries and they’re well characterized. And the FDA agrees: the vaccines cause blood clots. The vaccines cause heart damage. The vaccines cause neurologic damage. They also cause well-characterized immunologic and hematologic system damage.
This is in the peer reviewed literature. This is not equivocal. This is not a subject of controversy or debate. It’s in our literature.
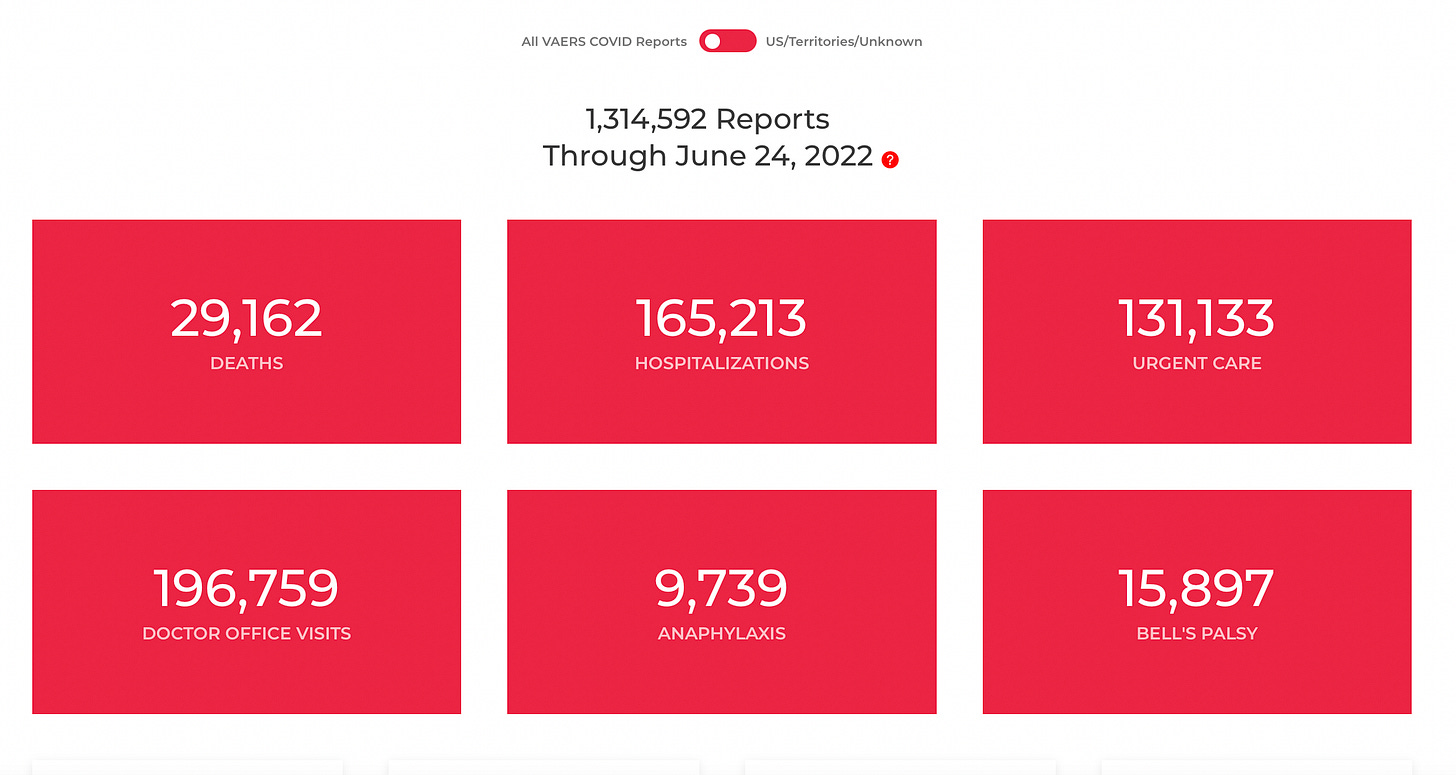
There are now brand-new diseases named after COVID-19 vaccine injuries. As of June 17th, 2022, our CDC VAERS system has been certified: 13,388 Americans who have died with the vaccine. Though either they have taken them electively or they were forced into it. That’s 13,388 people have lost their lives prematurely due to these vaccines.
The vaccines qualify by the Bradford Hill criteria, which is an organized set of criteria on causality, they qualify as causing these deaths according to these epidemiologic criteria.
I am a trained epidemiologist. I am an expert in applying these criteria. On a more probable than not basis, and almost certainly clear and convincing: these vaccines are causing death.
World Council For Health Calls For Global Recall of COVID Vaccines
This month the World Council for Health which represents 70 bodies worldwide has called for a global recall of all [COVID-19] vaccines. Because worldwide 40,000 deaths that these safety databases across the world—forty thousand in the big ones—VAERS, the Yellow Card System, the VIGI Safe, and the EUDRA system. Forty thousand deaths with the vaccines. Unacceptably high.
Typical standard for any biologic product is 50 deaths, pull it off the market. Something’s gone wrong. Fifty… not 40,000!
So when there is a global recall by an international organization this committee ought to be having emergency meetings.
What are we going to do? A worldwide body has called for these to be pulled off the market. They’re still giving it. You just heard from the pharmacy director ahead of me, he’s still giving them out. When there’s a worldwide recall, there should be some committee meeting. So you have it down. I mean, you can tell something is going wrong here, that we are in trouble in terms of vaccine safety.
Vaccines Not Effective Against Omicron
Dr. Robert Malone has covered vaccine efficacy, which has largely waned.
I will just tell you that the CDC told us, as of December 10th, 2021 with the Omicron strain, 79 percent of people with Omicron were fully vaccinated. That is prima facie evidence that the vaccines have completely failed against Omicron variant.
It’s inverted now: The vast majority of people who are sick with COVID-19 and in the hospitals worldwide with the Omicron variant were fully vaccinated.
Madame Chairwoman: I have a quick question for you about when you talk about the worldwide reports and the worldwide rejection global recall. Is Congress doing anything about it?
Dr. McCullough: To my knowledge, no U.S. body has reacted to this worldwide call at all. So it’s not, it’s obviously a failure at the state level and at the national level. It’s essentially in oblivion. It’s in oblivion.
Widespread Censorship of Physicians and Others
Final set of comments: physician censorship and reprisal.
It is clear now that in the area of Covid that it’s open season for censorship and reprisals, not just of physicians, but of nurses and patients and family members and others. And the censorship is because there is a global effort to mass vaccinate the population every six months, and anything that would deter from that is going to be censored.
So if a family member has lost a loved one after the vaccine, that event, if it’s written somewhere what have you, is censored. We have widespread censorship in the medical literature now, in social media, and even in oral presentations.
I presented here on May 10th, 2021. Five statements that I made here under oath are now subject of censorship and professional reprisal by the American Board of Internal Medicine.
Every single statement I made just in my written remarks and my prepared remarks is cited.
The American Board of Internal Medicine, the Texas Medical Board—they don’t have a monopoly on the truth.
No one holds medical truth.
There are always two points of view on everything, or more.
And so Senator Johnson has stepped in and called the American Board of Internal Medicine out to have a roundtable discussion on what’s going on now is a giant sweep through the federation of medical boards, through the American Board of Internal Medicine, American Board of Family Medicine, etc., and to have an open conversation.
They have not responded. In fact, they’ve doubled down and said they’re joining forces with the American Medical Association, again, in an effort to inflict reprisal on physicians as myself who are attempting to help patients through COVID-19 respond to the pandemic in terms of our patient care, our scholarship, and our research. And also give patients a fair appraisal on a brand-new set of experimental genetic vaccines, which for some patients now represents a mortal threat to them. And we must have certainly a conversation about the risks and benefits.
So, I think right now the most important thing that this committee can do is this committee probably ought to have a working group on censorship and reprisal at the professional level.
Doctors, nurses, patients who under the watch of DHHS are actually incurring their constitutional rights being stripped away from free speech. What is going on in this state actually impair medical progress. Remember, medical progress will not happen unless there is a roundtable discussion on something.
What–several speakers a few minutes ago, he talked about a conversation between some doctors and a doctor who wanted to prescribe ivermectin. That conversation to me didn’t seem very fair and balanced. It seemed like a disciplinary conversation. There is no disciplinary conversations in a brand-new novel coronavirus. This is all about getting the patient better.
Patient Rights Matter
The other thing I heard in that conversation is a very very important act of censorship or a violation of medical ethics is Dr. Bob Hall presented a case where a family member wanted the discussion about ivermectin of a patient in the hospital. There is a principle of medical ethics called shared decision-making.
When you’re a patient in the hospital you actually have a right to discuss what you want to have happen with your body. If you’re taking a medicine as an outpatient and you want to take that as an inpatient that’s called medication reconciliation. You have the full right to do so. No doctor can lord over you and say, “No you can’t have that medication.”
If you’ve had a fair balance discussion and the drugs, like ivermectin, hydroxychloroquine, are supported by hundreds and hundreds of clinical trials, they’re in dozens of government guidelines elsewhere in the world as first line therapy. Any American, any Texan, has the right to receive these drugs in the hospital when they engage in discussion with their doctor.
And under no circumstances should any doctor refuse a patient shared decision-making and their own personal autonomy. It’s unethical, it’s immoral and from a clinical perspective it’s illegal.
Source – https://jennifermargulis.substack.com/p/40000-deaths-but-no-recall