
In the first part of this series, I discussed how diseases frequently emerge that before long affect many people, and how in many cases conventional medicine cannot acknowledge what happened. Instead, these diseases will often be labeled as “syndromes,” a designation that is often a result of politics. This is because those syndromes often arise from a recently introduced environmental toxin that no one in power is willing to blame for causing a catastrophe.
In the second part of this series, I discussed how vaccines, particularly the Diphtheria Pertussis Tetanus vaccine, have had a large number of issues, one of which was causing sudden infant death syndrome. Despite a century of evidence clearly showing DPT causes SIDS however, the cause of SIDS remains “unknown.”
In the past, unless you were a parent who lost a child to SIDS, deaths from vaccines were typically not an issue of immediate concern. However, now that the spike protein vaccines are triggering the emergence of sudden adult death syndrome, this has become an issue that affects everyone. Because of this, I believe an exploration of how vaccines can cause sudden death is important.
To do so, we must first cover some foundational concepts that are not normally taught within medicine. This article will hence be the longer end, and I believe it is one of the most important things I will write here so I sincerely thank you for taking the time to consider its contents.
If you can’t understand some of the concepts listed here that is fine; all of them are essentially different ways of explaining the same thing that I have to present in order to justify my hypothesis, so just focus on what makes sense to you. In the future that will no longer be necessary and I will publish an abridged version of this article.
Early Observations
When COVID-19 started, I began to receive a variety of reports from colleagues suggesting this virus did not behave like a typical respiratory infection. I was particularly concerned by their observations that various fluids throughout the bodies of COVID-19 patients became frozen or solidified (blood clotting is the most well-known example). All of this suggested the pathology of SARS-CoV-2 was in part mediated by changes in the physiologic zeta potential.
After I formed this hypothesis, the next question was “what part of the virus could account for its ability to collapse the zeta potential of the body?” Knowing that it would have to be a positively charged protein on the surface of the virus, I looked through each of the surface proteins and noticed there was a remarkable positive charge density on the spike protein that exceeded what had been found in SARS-CoV-1 (subsequently it was also discovered that further increases in the positive charge of the spike protein correlated with the increasing pathogenicity the SARS-CoV-2 variants).
After discovering this potential issue, I then learned that some of the COVID-19 vaccine candidates functioned by causing the body to mass produce the SARS-CoV-2 spike protein internally (at this time the toxicity of the protein was not understood, but it was suspected by some to play a key role in disease pathology). The potential effect on physiologic zeta potential was my initial reason for being highly concerned about the spike protein vaccines, and this concern significantly worsened when I later learned the spike protein shared an unusual degree of homology with human tissue (as this is a recipe for developing autoimmune disorders, the other frequent severe consequence of vaccination).
Since that time, although I have not yet found a study where the zeta potential of the spike protein was directly tested, I have found numerous studies that suggest the spike protein disrupts physiologic zeta potential. More importantly, I have observed a variety of therapies that restore zeta potential benefit both individuals with COVID-19 and those with spike proteins vaccine injuries, sometimes to a minor extent, and sometimes to the point they fully resolved an otherwise fatal disease process (the exact result largely depends on the specific therapy utilized and the exact issue the patient has).
All of that is a lot to unpack, and the purpose of this article is to explain exactly what all of that meant. Much of this was made possible by the work of Thomas Riddick and Andrew Moulden.
Thanks for reading The Forgotten Side of Medicine! Subscribe for free to receive new posts and support my work.
Andrew Moulden
Andrew Moulden was a Canadian Ph.D. neuroscientist who focused on childhood development and acquired brain injuries, and then subsequently became a doctor specializing in neuropsychiatry.
During Moulden’s clinical training, he came across numerous cases of young children who developed textbook neurological signs of strokes none of his colleagues recognized, and over time, he noticed some of those children would subsequently develop severe neurological disorders (such as autism or losing the ability to speak). As Moulden began to try and understand what could be causing all of this, it became very clear the initial strokes followed vaccination, sometimes within hours of a vaccine.
Previously, to explain the extremely cruel phenomena of medical gaslighting, I illustrated how well-intentioned doctors typically cannot see signs of a condition unless they were specifically trained to look for them. I believe this is primarily because relatively few doctors have the perceptual capacity to continually monitor the entire patient in front of them (which is necessary for many diagnostic insights) and instead must filter the patient through the diagnostic algorithms they were taught in their medical education.
Despite my acceptance of this fundamental limitation in medical diagnosis, it still astounds me that Moulden was one of the first to realize the same subtle signs doctors and particularly neurologists are taught to look for in adults to assess for signs that a stroke occurred also should be recognized in children. Instead, doctors only recognize overt signs of a pediatric stroke such as a large facial droop. Because doctors consistently fail to diagnose these less obvious strokes in infants, we are left with a variety of conditions that are written off as the infant being “cute,” or having a disorder of unknown cause (for example, esotropia, a fancy term for the eye turning inwards, affects 2% of the population).
One of the major challenges in science is making the “invisible” visible so it can be researched in a reproducible fashion, and typically the smaller something is, the more challenging this is to do. This I believe is the fundamental issue underlying the belief some have that viruses do not exist (because viruses are so small, observing them almost always requires a certain degree of inference).
One of the great things about neurology is that this invisibility can often be bypassed because when there is a problem somewhere in the brain (commonly as a result of impaired blood flow to that region) the corresponding function that region is responsible for will become disrupted as well. With appropriate training, a physical examination can often detect that disruption and determine exactly where a stroke has occurred. In most cases, the status of the cranial nerves provides the most accessible window for evaluating the brain, which is why all medical students are taught to superficially evaluate them (unfortunately they rarely perform the in-depth examinations that can tell you much more about the patient).
Most nerves that travel throughout your body (not counting those that remain within the central nervous system) originate from your spinal cord. The twelve cranial nerves are the exception and instead originate from the brain (with most originating in the brainstem).
The cranial nerves within the brainstem are vulnerable to strokes because of the anatomy of the circulatory system. In most cases, the tissues of the body (especially those that cannot tolerate an interruption of their blood supply like the heart and brain) have multiple sources of blood so that a disruption in one of their blood vessels is unlikely to cause a critical failure. Watershed areas denote locations where that redundancy does not exist, and as a result, strokes are much more common within the watershed areas.
Many of the cranial nerves in the brainstem originate in watershed areas, which allows their dysfunction to serve as an early warning sign blood flow is being disrupted throughout the brain. Additionally, the blood vessels that feed the back of the brain where these cranial nerves are located are narrower than those that feed the front of the brain (20% of cerebral blood flow originates from the back, 80% from the front). This is important because an increased thickness of blood will always reduce blood flow, and has the greatest impact on smaller blood vessels, such as the narrower arteries that feed the brainstem.
The cranial nerves that typically indicate the presence of vaccine-caused micro-strokes (due to their less robust blood supply) are those responsible for controlling the movement of the eyes and facial muscle tone. The three nerves most commonly affected by vaccine microstrokes are as follows:
•Cranial Nerve VI: This nerve is responsible for controlling the muscle that makes the eye look outward. When a deficit is present, the eye will often look inwards at rest, and when both eyes look from side to side, the affected side will often jump rather than moving in a slow continuous motion like the unaffected side (this happens quickly and can require a slowed down recording to recognize).

•Cranial Nerve VII: This nerve is responsible for controlling most of the muscles in your face and one of the most commonly associated issues with this nerve is Bell’s Palsy, where one side of the face droops downwards. Less easily recognized facial changes can also occur, such as a flattening of the nasolabial fold, or the development of a crooked smile. In a previous article that discussed Justin Bieber’s recent vaccine injury, I showed how historical photography demonstrates that the age of vaccination has caused widespread cranial nerve damage that has resulted in asymmetrical faces going from being the exception to the norm.

•Cranial Nerve IV: This nerve serves as a leveler that maintains the eyes at an equal height. When there is an issue, individuals will typically tilt their heads to one side to restore the levelness between the eyes (asymmetries in the heights and vertical motion of the eyes can also be observed). Once you know how to look for this, it is very easy to spot.

Moulden also observed problems would arise in other cranial nerves, and his preferred test for these issues was to monitor blinking (either spontaneously or when provoked through a reflex). Once those nerves had become damaged, the eyes would no longer blink evenly. This difference is best observed on a slowed-down video recording and is also valuable diagnostically because it is very difficult to fake this dysfunction.
As Moulden continued to observe these microstrokes, he realized the cranial nerve dysfunctions indicated strokes were likely happening in many other watershed areas (such as the peripheries of the internal organs or the center of the brain that controls speech). Some of the key pieces of evidence to support his theory were:
•Moulden was able to review at least one autopsy study of a child who had died from congenital rubella (the R in MMR and a disease that can sometimes cause autism independent of vaccination or many other birth defects if the mother is infected while pregnant). In these studies, Moulden found that in addition to strokes occurring within the brain, signs of strokes were also found throughout the internal organs (which have watershed areas at their periphery).
•With the two vaccines that were best known for causing severe reactions (HPV and anthrax), Moulden observed a very similar disease process to what he had seen in children happen in teenagers and young adults.
•One of the most striking examples showing the effect of vaccination on circulation were children of soldiers who received the anthrax vaccine and were born without limbs (thalidomide was notorious for this and instead did so by blocking the formation of new blood vessels).

•Moulden observed many cases of these same neurodegenerative processes occurring in the elderly after vaccination (like many of the readers here, I have come across numerous cases of permanent dementia rapidly appearing after the spike protein vaccines). Moulden thus believed Alzheimer’s disease was another manifestation of this same disease process and my mentors have observed it often improves once cerebral fluid circulation is restored.
•Moulden observed numerous individuals with psychiatric disorders (such as schizophrenia) who also shared this characteristic cranial nerve damage. A major shortfall within conventional medicine is not recognizing that neurological damage creates psychiatric issues, and as a result, when patients present with medical injuries that also affect their nervous system, the emotional changes they undergo is labeled as the cause of their illness rather than a symptom of it.
With time, Moulden recognized that many different diseases (e.g. vaccine injuries, complications of infections, autoimmune disorders, and neurological conditions) appeared to share the same cause — pervasive microstrokes throughout the body.
He also noted that certain microbes tended to disrupt the blood flow in specific regions of the body (this is a foundational belief within Chinese Medicine) and that the responses to the same blood flow impairing process could produce entirely different responses in different individuals.
To this point, Moulden liked to cite the case of two identical twin boys who shared the same disrupted placental blood supply during prenatal development: one then developed features of autism, and the other developed learning disabilities and language problems.
All of this raises two major questions. What could be causing these microstrokes, and how do you treat them?
Moulden eventually concluded a non-specific response to toxins and infections was responsible for a wide range of diseases, and that the fundamental error of our medical model was it being focused on the countless causative agents of disease rather than the universal response itself (this was the basis for Moulden’s critique of germ theory). Moulden announced he had developed a means to address this response, but unfortunately died in suspicious circumstances shortly after the announcement, leading to his work being lost (this is a key reason why my mentors have not published on this topic and part of why I write anonymously).
Fortunately, I had independently researched this topic for years before I came across Moulden’s work, and was familiar with many of the same primary sources he used (along with others I suspect he did not). Additionally, following his passing, I learned friends of mine knew Moulden and I have since been able to glean additional insights into what he was working on.
Note: Although minimal testing have been conducted for the biodistribution of the spike protein vaccines and it is not known if they directly attack the cranial nerves, it has been shown that the AstraZeneca vaccine accumulates and persists within the sciatic nerve.
Scientific Distortions
When you study the history of science, one of the fascinating things you will discover is how many important scientific discoveries fell to the wayside, either due to politics, chance circumstances, or financial interests in promoting one scientific model over another.
Although I believe viruses like SARS-CoV-2 “exist,” one reason why I have a great deal of sympathy for that perspective it does not exist is that one of its foundations (that the flawed conception that viruses exist has completely distorted centuries of science) is analogous to what can be found in many other areas of science. However, while I believe important scientific truths can easily be erased, my faith also holds the belief that if something is true, it will continually be rediscovered throughout human history and when the time is right, emerge back into the public consciousness.
I have always loved puzzles (or puzzle games), and much of my passion for medicine comes from the infinite complexity of the body and the complexity of the puzzles it can create. Some doctors follow my philosophical orientation, but most prefer to work with clearly established treatment algorithms, and depending on the disease either type of doctor will be more appropriate for helping the patient.
Because there is so much complexity to the body, “models” are needed to simplify what is going on into a more manageable picture, and I believe this is often the reason why the medical profession collectively rejects models that require embracing complexity and uncertainty. Most of the traditional holistic medical systems utilize different models for understanding disease and I would argue one of the greatest shortfalls within modern medicine is the inability of physicians to recognize rather than modern medicine being an all-encompassing understanding of the body, it is simply another (albeit complicated) model that has been developed for making sense of the immense complexity of disease. This is also why conventionally trained doctors often have an immensely beneficial broadening in perspective after learning a holistic medical system and the alternative medical model it is based upon.
The conventional medical model likewise rests upon multiple scientific disciplines, but it is rarely recognized that we are biased to heavily prioritize only one of them. To be more specific, I believe the following scientific fields are crucial for understanding the human physiology:
•Biochemistry
•General (and organic) chemistry
•Physical chemistry
•Biophysics
However, while each model is important, in medicine, we almost entirely focus on the biochemical model. Many believe this is because the biochemical model is based upon the innumerable specific reactions that occur between proteins (such as enzymes or cellular receptors) and the endless number of substances that can affect them. Following that model establishes a paradigm where the root cause of disease can only be rationally addressed by producing patentable substances that target those proteins, and requires that each proposed medical approach prove itself within this paradigm. Following this model hence makes medicine become an incredibly expensive endeavor that always needs expensive research to map out new biochemical (or genetic) pathways and to develop new highly lucrative drugs that alter these pathways.
The other scientific models are also utilized within medicine, but typically are only utilized when needed for something the medical industry depends upon:
•Colloidal chemistry, the focus of this article and a subset of physical chemistry is critically important for normal physiology but is rarely considered in medicine, and one of the only times I can recall coming across this discipline recently was within the Pfizer EMA documents. There, a discussion could be found regarding the zeta potential of the lipid nanoparticles that was required for them to effectively traffic mRNA into cells.
•Although general chemistry is typically relegated to a few things like the acid-base balance in a hospitalized patient, many effective therapeutics have been developed that utilize the principles of general chemistry. In most cases, these therapeutics have a wide range of conditions they can be used for since they are not dependent on the molecular specificity inherent to biochemical therapeutics (which is likely why they were all discarded by the conventional medical system).
A major challenge with mRNA vaccine injuries was that the vaccine was engineered to resist the enzymes the body uses to biochemically destroy mRNA, hence leading to it producing toxic spike proteins in the body long after vaccination. Although an expensive enzyme that solves this issue may be engineered in the future, it must also be remembered the mRNA is incredibly fragile (hence why the vaccines degrade so quickly if they are not within the protective environment of the body), and it is quite likely a general chemical process the body can tolerate will prove successful in degrading the synthetic mRNA (I have already seen signs suggesting at least one can).
•If I had to choose one, I would argue biophysics is the most important scientific model for medicine. Conventionally, we only use it for certain billable medical procedures such as radiographic imaging of the body, electrical monitoring of the heart or nervous system, radioactive destruction of tissue, targeted destruction or stimulation of nerves, and shocking a heart back to life.
Many other invaluable applications of biophysics also exist, and before the Robber Baron monopolized medicine, were explored throughout America. Currently, research into these approaches occurs primarily within Russia, the former Soviet republics, and to some extent Cuba.
During the time of the USSR, each of those nations developed a robust research apparatus, but due to their economies becoming impoverished by the fall of the USSR, they subsequently could not quite afford the biochemical form of medicine (as it requires continually utilizing expensive pharmaceuticals). Medical approaches utilizing biophysics by contrast tend to be more universal and cheaper to implement, hence only making them politically viable in countries that now lack the wealth to fund modern medicine (Germany is an exception in this regard as the culture has always been very supportive of alternative medical approaches).
Strokes
Classically, three types of strokes can occur:
•A clot forms somewhere in the circulation and eventually arrives at a blood vessel it is too big to fit through and blocks it (an embolic stroke).
•A blood vessel ruptures and leaks blood into the surrounding tissue (a hemorrhagic stroke).
•Damage occurs to the endothelium (the lining of the blood vessel walls) and the protective response of the endothelium causes a blood clot to form at the site of injury (which can give rise to a thrombogenic stroke).
The SARS-CoV-2 spike protein is remarkably effective at causing all three of these to occur. I believe this is a consequence of the spike protein being highly disruptive to zeta potential, the endothelium having a high concentration of the ACE-2 receptors that the spike protein binds, and the positively charged spike protein being electrically attracted to the glycocalycx. The glycocalyx, is a massive network of negatively charged glycoproteins that protectively coat the endothelium and when this critical function fails, many circulatory diseases emerge (diabetes for example destroys the glycocalyx, which may explain why diabetics are so much more vulnerable to circulatory disorders and COVID-19).
Recently, I came across an excellent article on the genotoxicity of the spike protein and a study showing the (positively charged) spike protein enters the (negatively charged) nucleus, that to the best of my knowledge has no receptor for the spike protein. In addition to illustrating the cancer-causing potential of the spike protein, this study also illustrates how the spike protein’s charge causes it to attack many negatively charged parts of the body like the glycocalyx.

In addition to these three recognized types of strokes, there is also a condition known as a transient ischemic attack (TIA), where one develops clinical signs of a stroke that later improve, while signs of the stroke are rarely seen on brain imaging. Although TIAs are viewed as self-limiting episodes, they are also recognized to be prognostic of a severe stroke in the future.
Some, including Moulden, believed TIAs represented a fourth class of stroke and indicate dangerous impairments to the microcirculation are occurring. However, unlike the previously described types of strokes, these strokes are too small to see with the resolution of existing radiologic imaging technologies and thus not believed to exist.
Frequently in the history of science, an important hypothesis with strong evidence supporting it will be denied until visual proof can be found for the hypothesis:
•Previously, I discussed the story of Semmelweis, a physician who proved doctors were killing approximately 10% (yes 10%) of the women they delivered babies from by refusing to wash their hands after dissecting corpses prior to the delivery. Semmelweis received severe reprisals for suggesting his colleagues could be infecting their patients, and his ideas only came to be accepted once Pasteur showed germs existed under the microscope (although I support terrain theory, this story illustrates why germ theory is also essential and should not be discarded).
•Another parallel can be drawn to continental drift, a now widely-accepted model that despite strong evidence supporting it, was widely ridiculed by the scientific field. Tectonic drift only became accepted after the U.S. Navy was able to provide direct visual evidence of underwater fault zones required for the continental drift model.
Because these microstrokes cannot easily be seen, they hence fall into the same scientific black hole as the previous examples and when recognized, have been lumped under the nebulous umbrella of “TIAs.” Moulden then concluded they were caused by two phenomena, pathologic changes in zeta potential and the Moulden Anoxia Spectrum Syndromes (MASS for short and completely coincidently also sharing a name with mass formation).
Blood Sludging
A common question that arises in many conditions (such as infections, severe crushing injuries, burns, or cancer) is how the individual insult can cause severe sickness or death throughout the body. Since at least the 1700s, Western medicine has observed that in certain disease states, the blood will partially solidify or increase its viscosity (i.e. thicken), which in the 1800s was observed to result from blood cells agglutinating or clumping together (many terms including blood sludging described this process). Starting in the 1930s, advances in optical microscopy made these changes possible to study within living tissues, and researchers such as Melvin Knisely Ph.D. extensively studied blood sludging until the 1960s, after which it became another forgotten side of medicine.
In totality this research demonstrated that blood sludging appears to be a common phenomena the body has numerous adaptations to (e.g. the terminal pulmonary arterioles have evolved traps to catch small sludges). However, once a critical threshold of blood sludging is reached, those adaptations are overwhelmed and critical failures emerge (e.g. larger clots causing pulmonary embolisms are often fatal and a common cause of death following spike protein vaccination).
One of Knisely’s most important experiments involved studying the progression of malaria in monkeys. There, he discovered that the parasite killed monkeys by creating severe blood sludging that initially occurred in the smaller vessels, and that as it increased (and the monkeys moved closer to death), could also be found obstructing the blood flow of the largest blood vessels in the body.
For example, in the inferior vena cavas of these monkeys, he observed its bottom third was a solid sludge of blood cells infested with malaria, its middle third had slowly moving clumps of blood cells and its top third was free flowing plasma without blood cells. The presence of infected sludges potentially explain why infections can “reactivate” (Lyme with its biofilms is well known for doing this) as Knisely periodically observed longstanding blood sludges (which the immune system cannot enter) rupture and release infectious organisms into the circulations. Additionally, larger blood vessels have their own blood supply, and when those smaller vessels becomes blocked with blood sludging, the resulting infarction can often destroy the lining of the larger vessel, leading to many diseases including vasculitides.
Most importantly, Knisely also found that if he provided heparin (a commonly used anticoagulant) to the monkeys, it dispersed their blood sludging and allowed them to survive dramatically longer with an untreated infection. This survival (both in monkeys and humans) also provided a key piece of evidence to support Moulden’s hypothesis of the damage blood sludging caused to the brain:
“Those patients who survive in attack of real cerebral malaria always carry residual diffuse brain disease in the form of healed microscopic infarct’s (from microclots). This condition may be clinically so slight as to be unmeasurable or there may be evidence of diffuse cerebral involvement with general doling of the intellect.”
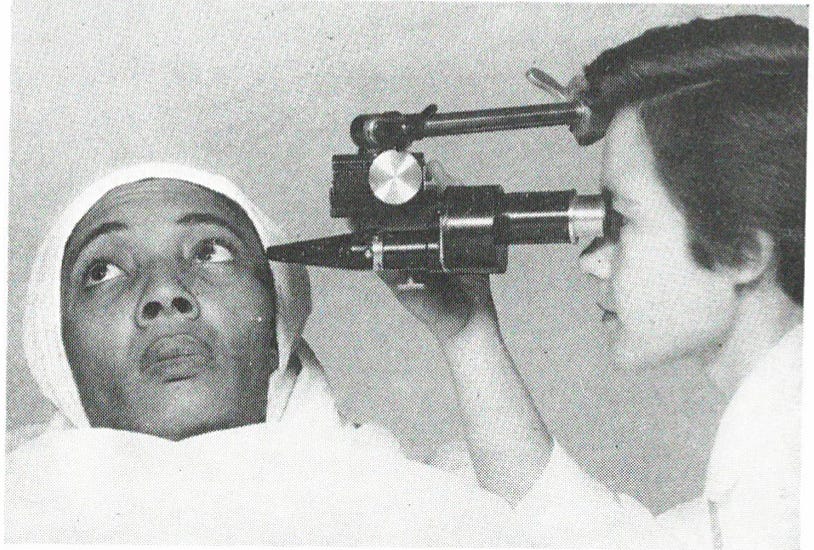
Most importantly, Knisely discovered that the blood sludging he could externally observe in the monkey’s eyes matched that found within their internal blood vessels (made visible through surgical incisions).
Recognizing the utility of this discovery, Knisely then developed a microscope for observing blood sludging in the eye (henceforth termed the sclerascope) and observed the eyes of countless individuals. With this tool Knisely (and others) found many different diseases (and certain toxins), appeared to cause their pathology through initiating widespread blood sludging and Knisely produced a grading scale for the varying degrees of blood sludging and pre-blood sludging that could occur that consistently correlated to disease prognosis.
Knisely (using a portable sclerascope) also found blood sludging was the most severe in hospitalized patients (I believe this is a large part of what leads people to require hospital care). Knisely also observed that certain agents such as hydroxychloroquine, atabrine, and quinine reversed blood sludging. This led him to suspected a significant degree of the benefit from hydroxychloroquine arose from it reducing blood sludging rather than it directly inhibiting the malaria parasite; I also suspect this property may account for its value in treating autoimmune conditions and COVID-19. Additionally, another popular home COVID-19 remedy, Alka-Seltzer, coincidentally contains many of the electrolytes Riddick (discussed later) found were ideal for dispersing blood sludging.
The blood sludging process is a consequence of blood cells agglutinating (clumping) together because once this happens, they stop being suspended in the plasma and with gravity settle to the bottom, creating sludged blood that is often deoxygenated and unable to flow. This issue was the most impactful within the smaller vessels where Knisely was able to observe it often completely blocked blood flow within the affected vessels (especially at branching points as the sludged blood would sink with gravity to the lower branch and block it, which was proposed to explain the changes patients with severe blood sludging experience as they change positions).
Moulden emphasized that these microstrokes would affect watershed areas of the body, including those in the periphery of the circulation such as tips of the fingers, toes, and nose (conventionally is that recognized as the cause of many conditions like frostbite). The best-known example of a disorders of impaired peripheral microcirculation is Raynaud’s syndrome, which in the conventional model is attributed to involuntary constrictions of the smallest arteries in the fingers and toes. I do not fully endorse this explanation because Raynaud’s syndrome often responds to treatments that address blood sludging, and has been repeatedly observed to onset following many of the older vaccines, COVID-19, and spike protein vaccines.
One “mystery” of COVID-19, is that COVID-19 patients can survive with blood oxygenation levels that are normally fatal. A key reason why many patients died in the early days of COVID-19 was that doctors did yet not realize COVID-19 patients could tolerate the dangerously low oxygen saturations they had and hence had a greater risk than benefit of being ventilated (which was then further worsened by a severe shortage of personnel who were sufficiently trained to safely manage ventilators).
I am almost certain this medical mystery resulted from COVID-19’s blood sludging being sufficient to partially freeze the blood flow in the smaller peripheral vessels, including those in the fingertips where blood oxygenation, through a wonderful application of biophysics, is almost always measured. Because this sludging prevented many of the red blood cells there from returning to the lungs, those cells were stuck in a deoxygenated state and thus created a low blood oxygenation reading.
In most cases, peripheral blood oxygenation matches the central blood oxygenation (which when low is fatal) but since the central blood vessels are so much wider, COVID-19’s blood sludging did not create the same obstruction within them. As a result, COVID-19 patients could be relatively well while simultaneously having a blood oxygenation reading that would normally suggest a high risk of death.
Presently two common diagnostic tests can show these changes in microcirculation. The first is the D-dimer test, which shows if microclotting is occurring throughout the body, but typically lacks diagnostic utility due to the large number of conditions that can elevate D-dimer levels.
The second is the erythrocyte sedimentation rate (ESR) test, a test that evaluates how quickly blood cells will settle to the bottom of plasma. This test turns positive in some inflammatory (typically those of an autoimmune nature) conditions and is thought to result from positively charged proteins that are released in inflammatory states (erythrocyte zeta potential is also considered but not conventionally viewed as the primary factor influencing the test).
The ESR is also elevated in migraine headaches, an extremely common disorder for which the cause remains unknown, and which I would argue results from blood sludging in the head (migranes often respond to treatments that address blood sludging and one researcher has attracted a large following with a model that I would argue does just that). It should also be noted that many other disorders thought to result from blood sludging, such as menstrual irregularities (e.g. pain or clotting) and tinnitus, like migraines, are frequently a consequence of spike protein vaccination.
Another important discoveries Knisely made was that when blood is taken out of the body, a significant number of factors change how it sludges. When he specifically examined blood samples undergoing the ESR test, he observed a significant number of artifacts (e.g. you are much less likely to draw sludged blood and structures will form in the test tube that prevent the erythrocytes from settling) leading him to suspect it did not precisely correlate to what was observed within the body.
Additionally, anytime blood is removed from the body (excluding the rare individual with a disorder like factor XII deficiency), it will spontaneously clot. Almost all of the agents that are used to prevent this intrinsic blood clotting pathway from disrupting a blood draw also disperse blood sludging (e.g. sodium citrate), which makes blood sludging quite challenging to study outside of the body. However, despite these significant artifacts, clear changes can often still be observed in blood outside of the body.
In my medical practice, mostly to perform ultraviolet blood irradiation, I frequently draw blood that is mixed with a small amount of heparin and then dilute the blood in saline bags and have thus observed the behavior of many blood samples. I (and a few colleagues) have found that typically in patients who are quite ill, and in whom we suspect blood sludging is occurring, the blood is much darker, and in the worst cases will also have the erythrocytes separate from the plasma and settle to the bottom of the bag.
This sedimentation is rare and I have only seen it in patients who required house calls for COVID-19 (an elevated ESR has been correlated to severe cases of COVID-19). Similarly, many alternative health care practitioners will observe blood samples on slides and believe that if the red blood cells clump together in a rouleaux formation, this suggests systemic problems within the body (they often prescribe fairly complex things like customized diets in an attempt to address those issues). As you might expect, highly unusual changes have been consistently observed in slides examining the blood from spike protein vaccinated individuals.

(Many better pictures of rouleaux formations exist, but I wanted to share this vintage one from Knisely).
There are also approaches that can bypass the potential diagnostic artifacts that are created when blood leaves the body. Overall, I believe a sclerascope is the best approach for detecting blood sludging. My team is using this approach for studying COVID-19 vaccine injuries as we believe therapies that can be observed to improve the blood sludging within the eyes will also improve many other aspects of these vaccine injuries.
Outside of sclerascopy, I believe the best approach is to know the clinical signs of blood sludging and some of the findings we use in Western medicine can indicate the presence of blood stasis (you can easily deduce which diagnostic signs likely result from blood sludging). However, I believe Chinese medicine, a system that does not require technology to make a diagnosis, offers some of the most useful diagnostic tools. This is because “blood stasis” is a key disease condition within Chinese medicine and almost perfectly overlaps with each characteristic Western researchers attributed to blood sludging; the Chinese government has also funded research that proves the presence of blood stasis with modern instrumentation.
The first article I wrote on this substack showed how contrary to the commonly held belief, the smallpox vaccination campaign was an unmitigated disaster that worsened smallpox outbreaks, severely injured or killed many, and each time it failed, was more aggressively mandated by the government onto a more and more resistant public (which is relevant since that is also what has happened with COVID-19).
Following that article, I wrote a follow-up on the severe changes in health physicians of the era observed following smallpox vaccination, which I believe marked a pivotal moment in the decline of the health of the entire human species (many, including my mentors, have observed a continual decline in the vitality of the human species over the last 150 years which coincided with an explosion of neurological and autoimmune diseases that have gotten harder and harder to treat). Many of the common effects of the smallpox vaccine matched the symptomatology of blood sludging, and interestingly, although Chinese medicine has existed for thousands of years, the push for blood stasis to be considered a primary disease pattern only began 150 years ago following the smallpox vaccination campaigns within China.
Although Knisely was able to consistently observe the presence and consequence of blood sludging in many conditions, to my knowledge, he was never able to definitively establish what caused it (his best guess was that it resulted from the protein-like aggregates and strands he frequently observed in concurrence with sludgey blood and conditions like rheumatoid arthritis).
Zeta Potential
Most phenomena in the realm we inhabit are the product of an equilibrium where competing forces meet a state of balance. When a substance is mixed in a liquid, exactly what happens to it, especially if the liquid is water, is a fairly complex equilibrium process. In some cases, the substances do not mix and separate by density (e.g. oil floating to the top or water or sand sinking to the bottom) and in other cases, the substance completely dissolves (salt mixing in water is a classic example).
Commonly however, the mixing process results in the formation of a colloidal suspension (most liquid systems in nature are colloids). Here the mixed substance disperses into particles that evenly distribute themselves throughout the liquid and an equilibrium is established between the attractive forces (gravity and the inherent attraction between molecules known as the van der Waals force) and the dispersive forces (the electrical repulsion between the particles).
Colloidal stability (and the colloid being able to separate into the tiniest particles possible) in turn results from the dispersive forces outweighing the attractive forces.
A few factors besides the charge characteristics of the colloid itself can affect colloidal stability. These are the other electrically charged substances present in the water, the presence of a protective colloid like gelatin or albumin that prevents agglomeration (the body utilizes these to prevent abrupt colloidal agglomeration from occurring), and large molecules that block colloidal particles from contacting each other.
If a charged substance goes into water, it will attract water ions (a certain portion of water is always positively or negatively charged) that have the opposite charge and form a tightly packed layer around the substance. That layer will then attract a second loosely packed of water ions layer with the opposite charge (which thus matches the charge of the initial substance). Zeta potential represents the electrical charge difference between this second layer and that of the bulk water surrounding it.

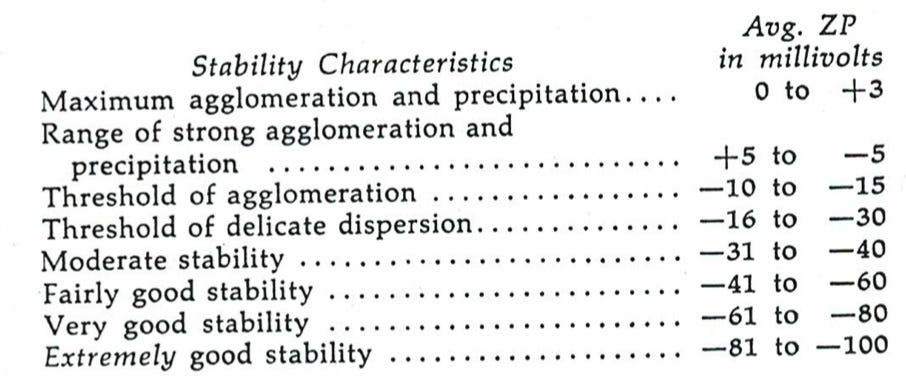
Almost all colloidal systems in nature depend the mutual repulsion of negative charges, and as a result, each requires a zeta potential that is negative enough to outweigh the attractive forces that are always present. Thus, as zeta potential moves to zero, agglomeration onsets, while as zeta potential becomes more negative, colloidal stability increases (Knisely’s consistent grading scale for blood sludging in the eyes was a reflection of how blood cells behaved at each zeta potential). Colloidal stability is critical for the body, so almost every surface inside the body is negatively charged to maintain a negatively charged colloidal system (for example see this paper on red blood cells and note that the source of their zeta potential is also what the spike protein preferentially binds in the glycocalyx).
An example to illustrate this concept can be seen in dust particles floating in the air that are made visible by sunlight illuminating them.

In this state, the positively charged dust particles repel each other and thus stay suspended in the air, but if they ever touch the floor, they take on a negative charge which causes them to stick together and never float up again. Negative ion generators likewise purify the air by having the negative ions agglomerate the floating dust particles, making them lose their suspension and sink to the ground.
Thomas Riddick
One of the early pioneers in the applications of zeta potential was Thomas Riddick, an industrial engineer whose firm was frequently required to adjust colloidal stability for clients. For example, clays are colloidal suspensions that need to remain suspended; if they agglomerate, they will clog the pipes they travel through.
Similarly, sewage is also a colloidal suspension that frequently creates issues for those who work with it. Because sewage is a colloidal suspension, treating it requires breaking its colloidal stability (termed flocculating) and causing the particles of organic matter to separate from the water and “sludge” together at the bottom where they can subsequently be removed.
Of the factors affecting colloidal stability, zeta potential is the easiest to modify (remember zeta potential is also dependent on what surrounds a suspended particle), and thus the primary focus of Riddick’s research. Changing zeta potential however is surprisingly complex for three key reasons:
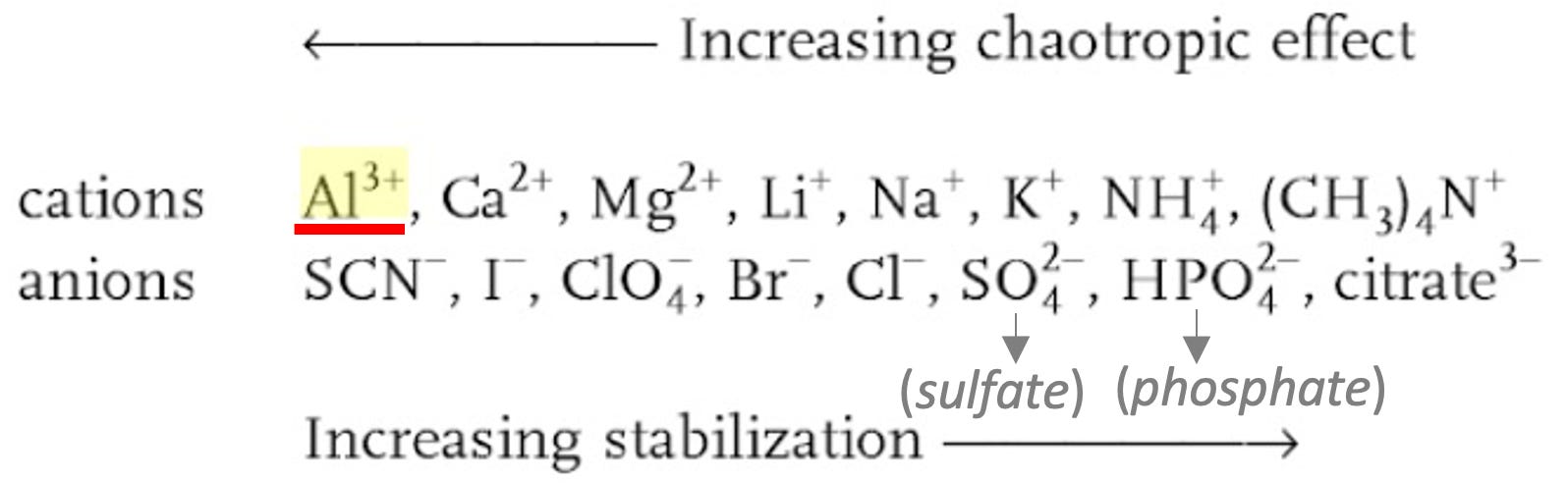
•Different ions have very different effects on zeta potential. This is largely due to their effect exponentially increasing with valence number (other characteristics also matter). As a result, +3 positively charged ions (cations) and -3 negatively charged ions (anions) have the greatest impact on zeta potential, while other ions like calcium (a +2 cation) will also have a significant influence (most physiologic decreases of zeta potential are mediated through calcium ion transport).
•Each ion that dissolves in water must originally be paired with an oppositely charged ion (e.g. table salt is sodium and chloride that separate in water), and that other ion also has a significant effect on zeta potential. Potassium, unlike sodium, does not significantly weaken zeta potential, so potassium salts (e.g. potassium phosphate) tend to perform much better than sodium salts when used for improving zeta potential.
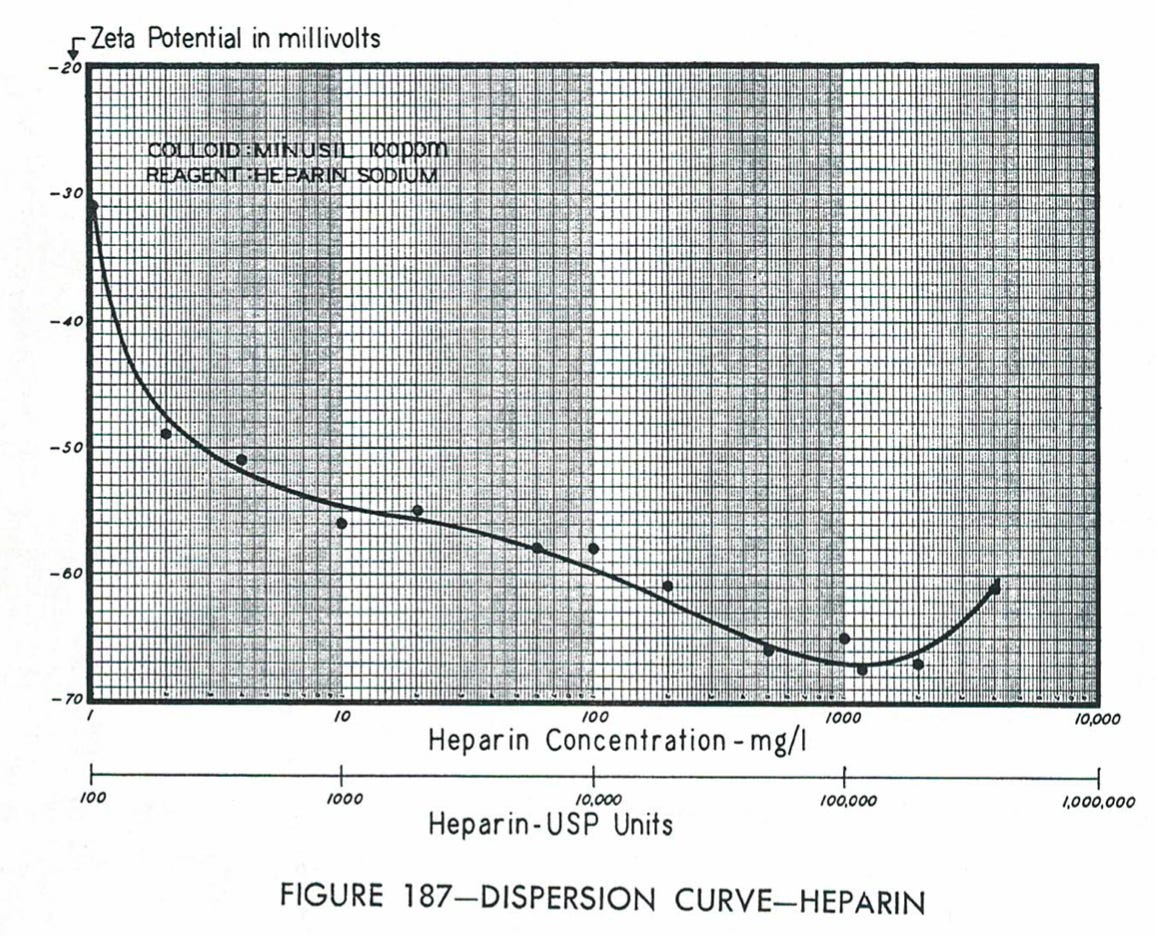
•Any negatively charged ion (anion) which improves zeta potential will follow a U-shaped curve as its concentration increases, which requires a concentration of the anionic dispersant to be used that does not reach the other end of that curve and worsen rather than improve zeta potential.
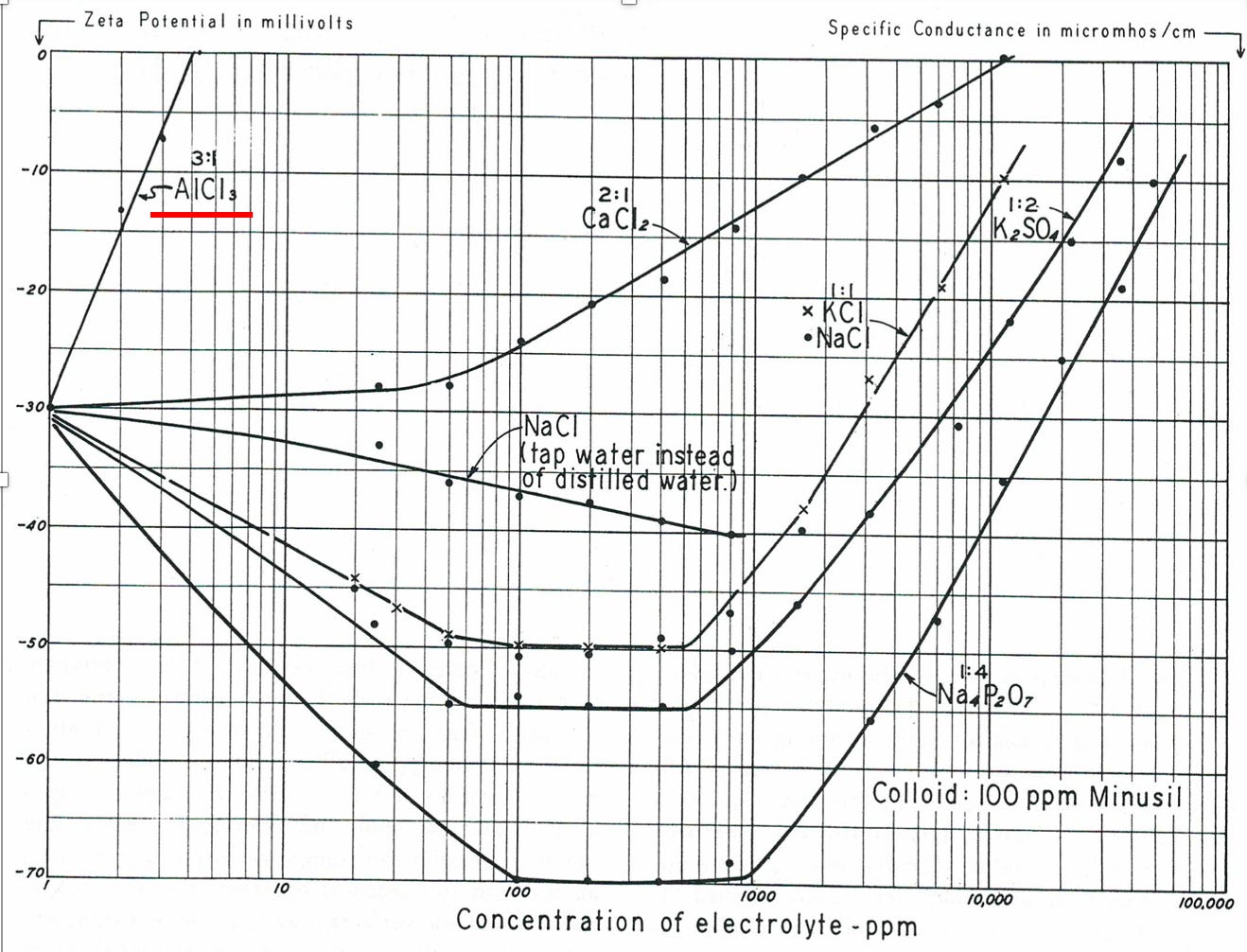
While reading the graph, pay attention to the logarithmic scale of the graph that is necessary to show the enormous differences in how different cations affect zeta potential. To put those values further in context:
In the cases where Riddick needed to agglomerate (flocculate) colloids, such as when treating sewage, he used aluminum, a +3 cation that was known to be the most effective substance for agglomerating colloids (this is standard practice in sewage treatment plants). In cases where Riddick needed to increase colloidal dispersion, he instead used the strongest anions (phosphate, citrate, and sulfate), which are also used throughout the body. Sulfate for example is the active ingredient in heparin (heparin has the highest negative charge density of any known biological macromolecule) and coats the surfaces of many tissues (including the glycocalyx). Riddick astutely noted many anticoagulants (heparin sulfate and sodium citrate) were also effective anionic dispersants.
I also believe a key biological function of sulfates is to create aggregates of gel-state water (this is why the glycocalyx is “slimy”), a form of water that plays numerous vital roles in human physiology and whose formation as best as I can determine depends upon the surrounding balance of anions and cations favoring the electronegative zeta potential human physiology depends upon. Gel-state water is an immensely important topic that will be covered in a future article. I and others also believe a key role of sunlight is to synthesize sulfates, which is why vitamin D, while helpful, is not an adequate replacement for sunlight.
Finally, when proteins are synthesized, they start as a long chain of amino acids. Due to a variety of interactions, proteins have with their surroundings (particularly water), these chains then “fold” into complex three-dimensional structures that allow the proteins to perform their intended functions. What is less appreciated about this process is that it means most three-dimensional proteins are colloidal suspensions (some scientific schools of thought now agree with this perspective) and the stability of their three-dimensional configurations is thus dependent on the same factors that elsewhere influence colloidal stability.
Note: I also believe the precise colloidal suspension process each protein undergoes is what allows them to “violate” the second law of thermodynamics and spontaneously decrease their entropy.
In 1888, a series was assembled by Franz Hoffmeister that showed how various substances would either stabilize folded proteins or denature and salt them out of solutions. Interestingly, his series was almost identical to the relative effects of specific ions on zeta potential.
As a result, ions that disrupt zeta potential can also cause protein misfolding, and I believe this is a key reason why aluminum is associated with Alzheimer’s disease (Alzheimer’s plaques are misfolded proteins that are often found with aluminum). This also my explain why the SARS-CoV-2 spike protein is associated with two other protein misfolding diseases: amyloidosis and prion diseases.
Zeta Potential and the Blood
Although I have many criticisms of modern medicine, I also recognize that it has had a profoundly positive impact on our modern lives and has solved many problems that plagued humanity for eons. In many cases, it is difficult to even conceive of what life would be like if we still faced those problems, and oftentimes developing those solutions we now take for granted required an immense amount of work that involved going down many dead ends and conducting many disastrous experiments.
At the time Riddick was alive, most of the approaches we now use for heart disease did not exist, and various common heart conditions like Riddick’s were a death sentence. This motivated Riddick to independently develop a solution to his disease, and he had the insight “what if blood is just another colloid (specifically blood cells suspended in plasma) that follows the rules I have developed from my industrial work with colloids?”
Before long, Riddick was able to establish that the process which caused blood sludging to occur was electrical, and through utilizing the anionic dispersants he had previously utilized for industrial applications, he was able to reverse blood sludging (I will also note aspirin, a well known anticoagulant, acetylates proteins and by doing so creates a negative charge). In addition to the anionic dispersants, Riddick also experimented with a few other effective approaches for restoring physiologic zeta potential such as consuming raw egg albumin mixed with distilled water.
All of this led him to postulate the initial step in blood clotting was blood agglomeration. This is extremely important because treating the agglomeration provides a way to “anticoagulate” the blood without incurring the risks inherent to any anticoagulant therapy (and also explains why things like dehydration or not moving for long periods are known to cause blood clots). Riddick later discovered the body keeps its zeta potential slightly below the agglomeration threshold, which allows it to clot where needed, but simultaneously makes it quite likely the countless modern disruptions to zeta potential (which our species has not yet evolved to handle) will also cross that critical threshold.
In dermatology, a commonly encountered issue is a wound on the skin that will not stop bleeding after skin surgery. One of the most common approaches in these instances is to apply aluminum chloride onto the skin as this agglomerates the blood and therefore begins the clotting process to stop the bleeding (in this context aluminum is viewed as a protein coagulant). This application provides a vital illustration of what occurs anytime there is a physiologic loss of zeta potential (extreme heat or cold can also cause agglomeration and modern surgery relies on this principle when cutting tissue with electrically heated instruments so that bleeding is prevented through coagulation).
With further study, Riddick found the degree of blood sludging or loss of physiologic zeta potential significantly varied from person to person, and Knisely’s grading scale for blood flow in the eyes could be used to accurately predict who was at risk of an arrhythmia, a stroke, or a fatal heart attack. Most importantly, Riddick discovered that once the colloidal dispersion of the blood was restored, heart arrhythmias normalized and circulatory problems greatly improved.
Riddick also discovered a primary function of the kidneys was to excrete the cations that destroyed physiologic zeta potential, and that when these cations were in excess, they could trigger cardiac episodes the kidneys would work in overdrive to correct (this likely explains the belief in Chinese medicine that the kidneys control the heart). This clearance seems to peak at night (likely from cations leaving the tissues and entering the bloodstream) and I have had a few experiences where I ate a lot of salty food before bed, woke up suddenly in the middle of the night with a fast heart rate and a feeling of being completely dried out inside which persisted until I drank a few glasses of distilled or reverse osmosis water (these are the two available forms of deionized water; any other form of water I tried did not work).
In these instances, I also observed I had unusual and highly conductive urine (this the easiest way to test for how many cations the kidneys are excreting). Riddick had more severe incidents of what I experienced, and by saving his urine for analysis during one episode, was able to show the kidneys had frantically worked to correct his zeta potential by excreting dangerous cations like aluminum.
As individuals age, the kidney’s ability to maintain zeta potential declines (Moulden hypothesized this was due to microstrokes in the peripheral watershed areas of the kidneys and Knisely produced videos showing blood sludges halving the kidney’s blood supply and plugging many of its filtration units). This decline makes the elderly much more susceptible to sudden influxes of positive charges and I am now of the belief a primary cause of aging is the gradual loss of the kidney’s function to maintain zeta potential (and to a lesser extent from albumin declining with age).
As Riddick attempted to deduce why unhealthy blood zeta potentials were so common (he found them in the majority eyes he looked at), he realized our society had contaminated the food supply with cations that were destructive to zeta potential (the first head of the FDA fought to stop aluminum from entering general use but was muscled out by industry) .
Examples included:
•Potassium being replaced by sodium in most processed foods
•Aluminum being used in most municipal water systems
•The widespread use of aluminum kitchenware
•Aluminum being added to many foods (e.g. most salt has aluminum added to keep it from caking, which amongst other things I believe this is why salty meals can cause heart failure exacerbations)
•Many medications like antacids being full of aluminum and other cations
•Many foods being stored in metal cans (acidic foods leach these metals) that are often aluminum.
Riddick also performed experiments that showed consuming water stored in aluminum significantly impaired microcirculation and for this reason, I will never drink anything from an aluminum can. Similarly, I have seen a few cases of patients with deficient zeta potentials having strokes a few hours after eating a meal that was cooked in aluminum.
Lastly a more disappointing note for those of you who drink, Riddick also found excessive alcohol consumption induced intravascular coagulation (it his research, two 2oz drinks of 90-100 proof seem to be cut off for triggering this).
Microbes and Zeta Potential
One of Riddick’s most interesting discoveries was that the bacterial metabolism of proteins would consistently lower their zeta potential, which he theorized was due to the decarboxylation reaction that occurs during the bacterial metabolism of protein (decarboxylation removes negative charges that would otherwise suspend these colloids). Many sewage treatment systems (e.g. septic tanks) work under this principle, as over time the bacteria within destroy the colloidal stability of the organic matter suspended in wastewater and cause it to separate from the water and sink to the bottom.
Because of this observation, Riddick also began assessing how zeta potential changed in human beings during periods of acute infections. In these cases, much like Knisely had previously seen in the eyes of his acutely ill test subjects, Riddick consistently observed a decrease in physiologic zeta potential occur during an infectious condition. In addition to their metabolism of human proteins, I believe this phenomena is also due to pathogenic organisms having a positive charge as it allows them to adhere to the negatively charged cells of the body (which likely helps to explain the universal applicability of oxidative therapies).
These observations were important because they provided a means to explain why the elderly are so much more vulnerable to infections like influenza. Sadly, it also likely explains their greater susceptibility to vaccinations—I still remember admitting one patient to the hospital who during her intake perfectly described a zeta potential collapse happening after a pneumococcal vaccination, including it being preceded by the kidney’s failed attempt to discharge the cations from the vaccine.
Regardless of who gets sick, infections consistently reduced zeta potential, but in the elderly who have a more impaired zeta potential to begin with, that reduction was sufficient to cross a threshold into serious illness. This process also explains why, as Moulden observed, vaccine damage is cumulative and more severe diseases onset as blood sludging progressively increases.
Although, as Riddick proved, the kidney can address many causes of impaired zeta potential, it typically struggles with disruptions caused by infectious microorganisms, particularly the smaller mycoplasma (which were instead eliminated by the spleen, liver and bone marrow). Lydia Mattman provided strong evidence for this, as she showed many of the stealth bacteria her research group discovered (once detected with the appropriate instrumentation), could be found to underlie many chronic kidney conditions.
Certain integrative doctors have had remarkable success in treating a variety of complex illnesses through lengthy antibiotic protocols, and I believe these successes are often a result of eliminating stealth bacteria that are impairing zeta potential. As antibiotics always have some degree of toxicity, I prefer other approaches to eliminate these organisms (e.g. oxidative therapies like ultraviolet blood irradiation).
In addition to the alternative broad-spectrum treatments for stealth bacteria, in some patients with impaired zeta potential, I have also had a great deal of success with specific German pleomorphic remedies that were developed to remove the pathogenicity of the stealth bacteria rather than directly eliminate them (one of the most well known researchers in this area, Gaston Naessens made a key observation that the foundational non-pathogenic form of these bacteria had a strong negative charge). Interestingly, one of these German remedies has also proven remarkably effective for reducing the blood sludging that commonly follows spike protein poisoning (it does not completely resolve the issue, but it is one of the only economical treatments I have found for this problem thus far).
MASS and Zeta
Vaccinations consistently contain many agents which are excellent at reducing the zeta potential of the body, particularly since aluminum, the most effective agent for reducing zeta potential is also the most widely used immune-stimulating vaccine adjuvant (I believe this is the reason why aluminum is such an effective adjuvant as attacking the zeta potential is a common characteristic of most pathogenic organisms and hence a likely trigger for the innate immune system). Moulden thus realized alterations in zeta potential could explain many of the injuries resulting from microstrokes he was seeing.
From studying the autopsies of children who had died from infections in the womb, Moulden also realized a second process occurred concurrently. Whenever an immunostimulatory event occurs, the white blood cells will migrate to certain capillaries so that they can exit them to enter the surrounding tissue. Because the white blood cells are much larger than red blood cells, if sufficient numbers of them are present within a capillary (particularly if partial blood sludging is already occurring there), their presence will block the flow of blood within the microcirculation. Moulden termed this process the Moulden Anoxia Spectrum Syndromes (MASS).
Thus, by reducing zeta potential and simultaneously provoking white blood cell recruitment through immune stimulation, the stage was set for vaccines to always cause varying degrees of harm. Additionally, certain vaccines like the HPV vaccine do so even more frequently because they utilize a specialized aluminum adjuvant designed to create a stronger immune response the vaccine needs to “work”. It should also be noted aluminum is the ingredient most directly responsible for the wide range of severe autoimmune vaccines cause (although the spike proteins likely will ultimately prove to be worse in this regard).
Moulden’s (and Riddick’s) model is immensely valuable because it provides a way to understand how:
•Vaccines, regardless of the design, consistently cause harm.
•Why vaccine damage is cumulative, as the microcirculation (and other fluid circulations) will worsen with each successive vaccine until a critical threshold is met where severe injury occurs.
•Why there can be so much variability in the injuries that are observed.
•How many infectious diseases can sometimes cause similar injuries to vaccines (but in almost all cases, the obstructions to blood flow are much worse following vaccination).
Shortly after I published this article I was contacted by a patient who had longstanding concerns over her body’s ability to tolerate a COVID-19 vaccine and had waited until Novavax was approved to vaccinate (she required the vaccine for work). After the first vaccination, she had a bit of a fever, but otherwise felt fine. Last night she received the second dose and this morning reported (quoted with her permission): “I have been up all night with my heart racing, fever, extreme body aches and a horrendous headache.” My hope is that I have shown how the concepts of MASS and Zeta explain exactly what happened to her.
Conclusion:
Poor zeta potential is one of the most common root causes of disease I encounter in my patients and “zeta potential” is the clearest correlate I have found to the ever-elusive concept of “health.” Books could be written on the profound importance of this subject, yet outside of a few applications like designing lipid nanoparticles, it is virtually unheard of in medicine (which is likely why the potential consequences of using positively charged lipid nanoparticles for the mRNA vaccines were never considered). A few leading members of the vaccine safety movement, along with some of the most talented integrative physicians I have met agree with these sentiments, but due to what happened to Moulden, none of them have spoken publicly on this issue.
Although many of the early pioneers of this concept established that poor zeta potential impaired blood circulation, which when addressed, can yield profound benefits for patients in countless areas, blood is not the only colloidal suspension in the body. Many other fluids in the body, also require a physiologic zeta potential, and when that becomes disturbed, many other diseases arise (e.g. I would argue many dermatologic conditions result from stagnation of the interstitium as they often responded to localized treatment of zeta potential).
The lymphatic system is the critical drainage system of the body, and when its circulation is obstructed by a non-physiologic zeta potential, countless diseases like edema, pneumonia (lymphatic stagnation is key in COVID-19 pneumonia), chronic infections, dementia, autoimmunity, and cancers initiate. Chinese medicine also commonly associates blood stasis with autoimmune disorders, and I am of the belief this is a result of the lymphatic stasis that often occurs concurrently with blood sludging.
Similarly, I have observed that patients with many of the common chronic disease that require years of integrative therapies (e.g. Lyme disease or chronic mold toxicity), almost always have signs of significant fluid stagnation throughout their bodies, and I can often connect it directly to their disease (e.g. mycotoxins and the Lyme bacteria carry a strong positive charge, which amongst other things is why I believe Lyme disease, something Justin Bieber had prior to his vaccine injury, causes Bell’s Palsy). In many cases, these patients can only get better if something is done to either restore their zeta potential or lymphatic circulation (otherwise antimicrobials will be often ineffective and overwhelm the patient) and since most integrative doctors are unaware of this concept, they often cannot help these patients.
A disease commonly seen in hospitalized patients, diabetic ketoacidosis (where the body becomes overwhelmed with excess levels of sugars and acidic ketones) further illustrates this concept. When these patients are treated in the hospital, they are always given insulin to lower their blood sugar along with potassium (as insulin moves potassium into cells). In addition to those two therapies, these patients are also always gives a saline solution under the rationale that without saline being administered, insulin cannot get where it is needed to reduce blood sugar levels.
Although this need for saline is commonly attributed to the patients being “dehydrated,” I believe it is due to sugar, when present at high levels, being a highly effective agent for disrupting colloidal stability (this is also why diabetics have so many problems with their peripheral microcirculation). Additionally, acidic environments disrupt physiologic zeta potential while alkaline ones support it (this is likely what accounts for many of the benefits attributed to health approaches that seek to alkalinize the body), so this impaired circulation is further compounded by the acidity of the ketones within the body.
Saline solution in turn is a somewhat effective means for restoring zeta potential (I have personally witnessed some profound examples that proved this concept to me) and it (or another fluid solution) is reflexively provided to almost all hospitalized patients despite almost no knowledge of its effect on zeta potential existing within the medical field. Because of this, I have long suspected the routine use of saline (and some other IV fluids) explains many of the benefits patients experience from hospital care. With saline, however, it is important to remember the U-shaped zeta potential curve Riddick described, as in higher concentrations, sodium chloride causes colloidal aggregation rather than dispersion.
Beyond hospitalized patients often having an immeasurable need for therapeutics that restore their zeta potential (which besides saline they rarely get), I am now of the opinion that many different holistic therapies all share the common mechanism of improving zeta potential.
One popular therapy, Earthing, for example, functions by electrically attaching oneself to the ground (a reservoir of negative charge) while sleeping so that the physiologic negative charge within the body can be restored (sleep, through melatonin sulfate and the redistribution of calcium ions, plays a key role in restoring zeta potential of the nervous system, but often cannot initiate if significant fluid stagnation is present).
Earthing’s proponents in turn argue that many modern health problems have arisen from us no longer being electrically connected to the ground. Almost every benefit I have seen attributed to Earthing (Earthing sometimes produces miraculous results for patients) reflects a restoration of zeta potential (which has been directly demonstrated in this study) and as one reader shared recently, it significantly improved his son’s Reynaud’s syndrome, while another shared it improved his COVID-19 vaccine injury.
Another fascinating therapy, negative ion therapy (breathing in negative ions) was researched for decades and proven to greatly benefit many challenging conditions. Most of this therapy’s benefits perfectly matched that which was to be expected from restoring the physiologic zeta potential. Unfortunately, despite decades of research proving it works, except for its ability to eliminate positively charged pollutants from the air by destroying their colloidal stability, negative ion therapy is typically viewed as pseudoscience, largely because there is no mechanism to explain why it could work (as the concept of physiologic zeta potential remains largely unknown).
Given the countless number of otherwise inexplicable diseases (particularly psychiatric and respiratory ones) which result from positive ions in the environment, I view it as a great shame this knowledge was lost. Common sources of positive ions include weather changes (which 25% of population is sensitive to), particulate pollution (e.g. cigarette smoke), EMFs (which can be observed in blood looked at under a microscope), ventilation systems (e.g. AC’s), furniture polishes and synthetic fabrics (many benefit immensely from wearing natural fabrics).
There are also many other therapies other there that also restore zeta potential and sometimes perform miracles for patients (e.g. ozone therapy or chelation therapy). Since their mechanism for doing so is less straightforward, I do not believe this science can be developed without a reliable way to measure each modality’s effects on the physiologic zeta potential. It is thus my sincere hope that in the future, direct measurements in the changes of physiologic zeta potential could be incorporated into the design of a variety of therapies, including those for treating spike protein injuries.
With the necessary background having been established, in the final installment of this series, we will review the existing autopsy studies of sudden deaths following vaccination and explore how the mechanisms described here along with many others can cause sudden death. Moulden for example has provided the best model I have ever come across to explain exactly how vaccines cause sudden infant death syndrome.
Source – https://amidwesterndoctor.substack.com/p/why-does-every-vaccine-often-cause