
A look at two recent studies
The New England Journal of Medicine published a study last week which looked at the effects of vaccination and previous infection on Omicron infection in children. The authors from the University of North Carolina, with a grant from the NIH, studied children aged 5 to 11 over a six month period. Whilst the study was limited due to possible waning effects of both vaccination and previous infection before the study period, it produced some interesting and concerning results.
First of all they looked at the effectiveness of the Pfizer vaccine against infection, according to date of first dose.
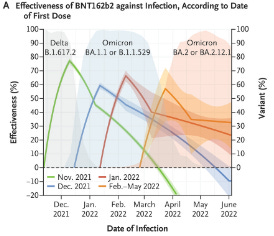
As you can see, vaccine efficacy peaks quickly but then also drops quickly. The green and blue lines actually enter negative efficacy, with the green line showing a -20% efficacy, 6 months after being injected. This means that vaccinated children were MORE likely to get infected than unvaccinated children. The authors continued to collect data until June 2022 so I have no idea why the green line stops in April 2022. Perhaps showing a more worrying negative efficacy in line with data from the UK Health Security Agency?
One of the most concerning results came in the next graph.

This compared previously infected and then vaccinated children (red line) with children who had not been infected and then were vaccinated (blue line). You would expect that previously infected children would have built up some natural immunity and therefore the red line would drop more slowly. However, both lines follow almost exactly the same path.
It looks as though vaccination has wiped out any natural immunity obtained from natural infection. Previous infection is irrelevant, the decline into negative efficacy after 18 weeks occurs at the same rate for both groups. Or is this some kind of Antibody Dependent Enhancement (ADE) showing up?
A similar story occurs in reinfection.
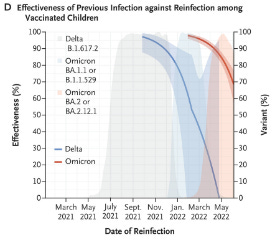
Vaccine protection is initially very high but drops quickly. Within 6 months vaccine efficacy reaches 0 and I would guess it follows initial infections into negative efficacy.
All of these charts show that vaccination produces an initial strong protection but it quickly disappears over 6 months. After this point it enters negative efficacy whereby the vaccinated individual is more likely to get infected than an unvaccinated person. How low does this negative efficacy go over time or does it return to zero?
But maybe this is just how the body works and the same thing happens in the unvaccinated? The next chart shows that this is not true.

The authors looked at the effectiveness of previous infection among unvaccinated children and the results were much different. Compare this chart to the ones above. Natural infection produces an initial 100% efficacy before slowly (compared with the vaccinated groups) dropping to around 50% after a year and half.
And finally, they looked at natural immunity versus vaccine efficacy against hospitalisation.
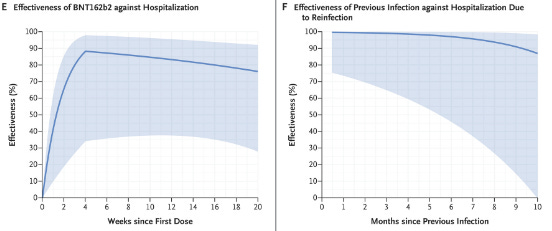
Chart E shows that peak vaccine protection against hospitalisation occurs at 4 weeks. This thin gradually falls to around 75% over the next 16 weeks. Previous infection, on the other hand, provides much stronger initial protection. It also drops much more slowly. Chart F shows that after 10 months (a different time scale than chart E), protection is still at around 85%.
Delving into the supplementary data shows that for the unvaccinated, fewer were getting infected with Omicron. Overall 90.1% of unvaccinated children got infected but this dropped to 81.7% during Omicron. Hospitalisation and death rates remained the same at 0.5% and 0.0% respectively.
However, for the 1 dosed infection rates rose from 1.6% overall to 2.8% with Omicron. Hospitalisation and death rates remained the same at 0.0% and 0.0%. For the 2 dosed, infection rates rose from 8.3% overall to 15.4% with Omicron. Hospitalisation rates also increased from 0.1% overall to 0.3% with Omicron. Death rates remained the same at 0.0%.
And finally another recent paper from John Hopkins University looked at COVID-19 vaccine boosters for young adults. This 50 page long paper looked at the risk-benefit assessment and five ethical arguments against mandates at universities.

The authors of this paper estimate that between 22,000 and 30,000 previously uninfected adults, aged 18-29, must be boosted to prevent one COVID-19 hospitalisation.
Looking at CDC and sponsor-reported adverse event data, they conclude that booster mandates may cause a net expected harm. They anticipate 18-98 serious adverse events, including 1.7-3 myocarditis cases. Furthermore, they anticipate 1,373 to 3,234 cases of >3 reactogenicity which interferes with daily activities. All to prevent one COVID-19 hospitalisation.
They add that due to the high prevalence of post-infection immunity, the risk-benefit profile will be even less favourable. Five ethical arguments are given against the mandates, including:
- no formal risk-benefit assessment exists for this age group;
- vaccine mandates may result in a net expected harm to individual young people;
- mandates are not proportionate: expected harms are not outweighed by public health benefits given the modest and transient effectiveness of vaccines against transmission;
- US mandates violate the reciprocity principle because rare serious vaccine-related harms will not be reliably compensated due to gaps in current vaccine injury schemes; and
- mandates create wider social harms.
Source – https://nakedemperor.substack.com/p/worrisome-new-data-vaccination-against