
Why the vaccines cannot protect against infection
A fundamental mistake underlying the development of the COVID-19 vaccines was to neglect the functional distinction between the two major categories of antibodies which the body produces in order to protect itself from pathogenic microbes.
The first category (secretory IgA) is produced by immune cells (lymphocytes) which are located directly underneath the mucous membranes that line the respiratory and intestinal tract. The antibodies produced by these lymphocytes are secreted through and to the surface of the mucous membranes. These antibodies are thus on site to meet air-borne viruses, and they may be able to prevent viral binding and infection of the cells.
The second category of antibodies (IgG and circulating IgA) occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream.
Vaccines that are injected into the muscle – i.e., the interior of the body – will only induce IgG and circulating IgA, not secretory IgA. Such antibodies cannot and will not effectively protect the mucous membranes from infection by SARS-CoV-2. Thus, the currently observed “breakthrough infections” among vaccinated individuals merely confirm the fundamental design flaws of the vaccines. Measurements of antibodies in the blood can never yield any information on the true status of immunity against infection of the respiratory tract.
The inability of vaccine-induced antibodies to prevent coronavirus infections has been reported in recent scientific publications.
The vaccines can trigger self-destruction
A natural infection with SARS-CoV-2 (coronavirus) will in most individuals remain localized to the respiratory tract. In contrast, the vaccines cause cells deep inside our body to express the viral spike protein, which they were never meant to do by nature. Any cell which expresses this foreign antigen will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ. We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. How and why such tragedies might causally be linked to vaccination has remained a matter of conjecture because scientific evidence has been lacking. This situation has now been rectified.
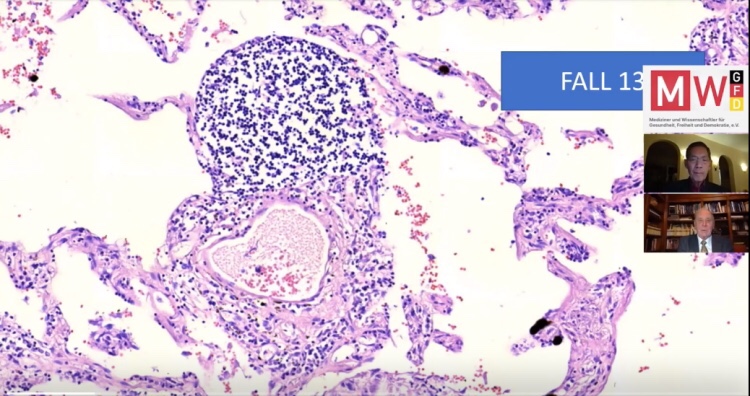
Histopathologic studies: the patients
Histopathologic analyses have been performed on the organs of 15 persons who died after vaccination. The age, gender, vaccination record, and time of death after injection of each patient are listed in the table on the next page. The following points are of utmost importance:
- Prior to death, only 4 of the 15 patients had been treated in the ICU for more than 2 days. The majority were never hospitalized and died at home (5), on the street (1), at work (1), in the car (1), or in home-care facilities (1). Therefore, in most cases, therapeutic intervention is unlikely to have significantly influenced the post-mortem findings.
- Not a single death was brought into any possible association with the vaccination by the coroner or the public prosecutor; this association was only established by our autopsy findings.
- The initially performed conventional post-mortems also uncovered no obvious hints to a possible role of vaccination, since the macroscopic appearance of the organs was overall unremarkable. In most cases, “rhythmogenic heart failure” was postulated as the cause of death.
Conclusion
Histopathologic analysis show clear evidence of vaccine-induced autoimmune-like pathology in multiple organs. That myriad adverse events deriving from such auto-attack processes must be expected to very frequently occur in all individuals, particularly following booster injections, is self-evident.
Beyond any doubt, injection of gene-based COVID-19 vaccines places lives under threat of illness and death. We note that both mRNA and vector-based vaccines are represented among these cases, as are all four major manufacturers.
The authors
Dr. Bhakdi has spent his life practicing, teaching and researching medical microbiology and infectious diseases. He chaired the Institute of Medical Microbiology and Hygiene at the Johannes Gutenberg Unversity of Mainz, Germany, from 1990 until his retirement in 2012. He has published over 300 research articles in the fields of immunology, bacteriology, virology and parasitology, and served from 1990 to 2012 as Editor-in-Chief of Medical Microbiology and Immunology, one of the first scientific journals of this field that was founded by Robert Koch in 1887.
Dr. Arne Burkhardt is a pathologist who has taught at the Universities of Hamburg, Berne and Tübingen. He was invited for visiting professorships/study visits in Japan (Nihon University), the United States (Brookhaven National Institute), Korea, Sweden, Malaysia and Turkey. He headed the Institute of Pathology in Reutlingen for 18 years. Subsquently, he worked as an independent practicing pathologist with consulting contracts with laboratories in the US. Burkhardt has published more than 150 scientific articles in German and international scientific journals as well as contributions to handbooks in German, English and Japanese. Over many years he has audited and certified institutes of pathology in Germany.