
These 2 papers by Cao et al. (NATURE) & Madewell et al. (JAMA) both in 2020, as well as the others I cite, told us all we needed to know ‘asymptomatic spread’ during COVID was a lie
Asymptomatic spread is virtually non-existent, and if this does occur, it is less than 1%. It is very rare and we have and had very limited evidence (and questionable) of this happening at all. We have no documented proof, no documented evidence of this occurring in any appreciable manner. Spread of pathogen will occur more surely when the persons are ill/sick with symptoms, especially if the symptoms function to expel the pathogen into the surrounding air. Having no symptoms or very mild symptoms reduces risk of spread and with no symptoms, spread is basically removed. If you have and had no symptoms, you do not transmit.
This means that all of the asymptomatic testing was never ever needed. None of it was ever needed and we used the flawed PCR test with the near 95% false positives (cycle count threshold over 24 detects viral junk, dust, fragments, not COVID virus; CDC set the cycle count threshold at 40), to shut down society. You do not mass test asymptomatic persons, you only test ‘symptomatic’ persons with strong clinical suspicion.
This is the same for SARS-CoV-2 virus and a recent BMJ publication pretty much sums it up that asymptomatic are rarely the drivers as it was thought to be. This is basic immunology and should not have changed for SARS-CoV-2 (COVID-19). I/we are being emphatic in saying there is and was no evidence of asymptomatic spread. We also recognize that one must be careful not to claim ‘zero’ as the evidence changes daily and rapidly and absence of documented evidence is also not a reason. It may just have not been studied yet or documented optimally. But we are confident enough based on the existing literature to also agree that ‘it is a dangerous assumption to believe that there is persuasive, scientific evidence of asymptomatic transmission’.
The basis for the societal lockdowns was that 40% to 50% of persons infected with SARS-CoV-2 could potentially spread it due to being asymptomatic. “But fears that the virus may be spread to a significant degree by asymptomatic carriers soon led government leaders to issue broad and lengthy stay-at-home orders and mask mandates out of concerns that anyone could be a silent spreader”. However, the evidence in support of common asymptomatic spread remains largely non-existent and we argue, was overstated and potentially was made with no basis.
A high-quality review study by Madewell published in JAMA (December 2020) sought toestimate the secondary attack rate of SARS-CoV-2 in households and determine factors that modify this parameter. In addition, researchers sought to estimate the proportion of households with index cases that had any secondary transmission, and also compared the SARS-CoV-2 household secondary attack rate with that of other severe viruses and with that to close contacts for studies that reported the secondary attack rate for both close and household contacts. The study was a meta-analysis of 54 studies with 77 758 participants. Secondary attack rates represented the spread to additional persons and researchers found a 25-fold increased risk within households between symptomatic positive infected index persons versus asymptomatic infected index persons. “Household secondary attack rates were increased from symptomatic index cases (18.0%; 95% CI, 14.2%-22.1%) than from asymptomatic index cases (0.7%; 95% CI, 0%-4.9%)”. This study showed just how rare asymptomatic spread was within a confined household environment.
From the nearly 2 million children that were followed in school in Sweden, it was reported that with no mask mandates, there were zero deaths from Covid and a few instances of transmission and minimal hospitalization.
In the UK, the ‘Scientific Advisory Group for Emergencies’ recommended that “Prioritizing rapid testing of symptomatic people is likely to have a greater impact on identifying positive cases and reducing transmission than frequent testing of asymptomatic people in an outbreak area”.
A study published in Nature in early 2020 by Cao et al. November 2020 (Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China) found no instances of asymptomatic spread from positive asymptomatic cases among all 1,174 close contacts of the cases, based on a base sample of 10 million persons. “There were no positive tests amongst 1,174 close contacts of asymptomatic cases”. AIER’s Zucker responded this way “The conclusion is not that asymptomatic spread is rare or that the science is uncertain. The study revealed something that hardly ever happens in these kinds of studies. There was not one documented case. Forget rare. Forget even Fauci’s previous suggestion that asymptomatic transmission exists but not does drive the spread. Replace all that with: never. At least not in this study for 10,000,000”. Haynes of Life site news reported similarly.
A study on infectivity of asymptomatic SARS-CoV-2 carriers was carried out by Goa at al. Researchers looked at the 455 contacts who were exposed to the asymptomatic COVID-19 virus carrier. They were divided into three groups: 35 patients, 196 family members and 224 hospital staffs. “No severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections was detected in 455 contacts by nucleic acid test”.
In this regard, the World Health Organization (WHO) also made this claim that asymptomatic spread/transmission is rare. This issue of asymptomatic spread is the key issue being used to force vaccination in children. The science, however, remains contrary to this proposed policy mandate. As an update that we say clearly is 16 months too late, the WHO on June 29th 2021 has now recommended no testing of asymptomatic persons. This is after trillions of $ have been sucked out of economies and many lives lost due to lost jobs and closures of societies and schools. Many people killed themselves due to the unscientific and illogical testing policy of asymptomatic persons.
Additionally, a high-quality robust study in the French Alps examined the spread of Covid-19 virus via a cluster of Covid-19. They followed one infected child who visited three different schools and interacted with other children, teachers, and various adults. They reported no instance of secondary transmission despite close interactions. These data have been available to the CDC and other health experts for over a year. As mentioned earlier, Ludvigsson published a seminal paper in the New England Journal of Medicine on Covid-19 among children 1 to 16 years of age and their teachers in Sweden.
A recent June 10th 2021 op-ed sheds more confirmatory light that asymptomatic spread was more a myth that a reality. Ballan and Tindall wrote “People presenting with symptoms of Covid-19 are almost exclusively responsible for transmitting SARS-CoV-2. Serious infection usually results from frequent exposure to high doses of SARS-CoV-2, such as health care workers caring for sick Covid-19 patients in hospitals or nursing homes and people living in the same household.
A person showing no symptoms of Covid-19 may test positive for SARS-CoV-2 on a PCR test, which doesn’t necessarily mean that they are infectious. There are four ways in which this can happen:
● The test may give a false positive result due to several faults in the testing process or in the test itself (the person is not infected);
● The person may have recovered from Covid-19 in the last three months (the person is not currently infected but dead debris of the virus are being picked up by the test);
● The person may be pre-symptomatic, i.e, the person is infected but still in the early stages of the disease and has not yet developed symptoms;
● The person may be asymptomatic, i.e. the person is infected but has pre-existing immunity and will never develop symptoms.
In asymptomatic individuals, the viral load is typically very low and the infectious period is also short in duration. They may still exhale virus particles, which another person may encounter. However, the overall likelihood of transmitting the disease to others is negligible. Thus, asymptomatic cases are not the major drivers of epidemics. As Dr Anthony Fauci of the US National Institute of Allergy and Infectious Diseases stated in March 2020: ‘In all the history of respiratory-borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person”.
Dr Clare Craig, a pathologist, and her colleague Dr Jonathan Engler have examined the research evidence behind the claim that Covid-19 can be transmitted by asymptomatic individuals. They wrote “harmful lockdown policies and mass testing have been justified on the assumption that asymptomatic transmission is a genuine risk. Given the harmful collateral effects of such policies, the precautionary principle should result in a very high evidential bar for asymptomatic transmission being set. However, the only word which can be used to describe the quality of evidence for this is woeful. A handful of questionable instances of spread have been massively amplified in the medical literature by repeatedly including them in meta-analyses that continue to be published, recycling the same evidence base.
There are three types of evidence for asymptomatic spread: studies showing people test positive while asymptomatic (the bulk of the work); studies measuring viral load and concluding from it that people with no symptoms can transmit virus; and studies showing actual transmission.
The first two are not proper evidence that spread can occur.
It is important to carefully distinguish purely asymptomatic (individuals who never develop any symptoms) from pre-symptomatic transmission (where individuals do eventually develop symptoms). To the extent that the latter phenomenon, which has in fact happened only very rarely, is deemed worthy of public health action, appropriate strategies to manage it (in the absence of significant asymptomatic transmission) would be entirely different and much less disruptive than those actually adopted.
Many early studies which purported to demonstrate the phenomenon of asymptomatic transmission were from China, yet the fact that Chinese studies are only published following Government approval must bring their reliability into question. Nevertheless, the high volume of these studies spawned significant salience of the issue within the medical community, and an assumption of the likelihood of asymptomatic transmission being an important contributory factor. There then followed a number of meta-analyses examining the issue of asymptomatic transmission which tended to aggregate and give equal weight to studies regardless of origin or quality. In this way, these meta-analyses, given undue credibility by their association with reputable universities, amplified minimal evidence of asymptomatic spread to an importance the data did not warrant.
A review of the literature has been submitted to the BMJ and is included here as a preprint. In it the papers most frequently cited in support of the existence of asymptomatic transmission were examined. Despite our criticisms of the sources of the data above, we did in fact find only six case reports of viral transmission by people who throughout remained asymptomatic, and this was to a total of seven other individuals. However, all of these were in studies with questionable methodology.
These were: In Italy, two asymptomatic cases allegedly passing the virus to two others, in Brunei, two asymptomatic cases allegedly passing the virus to three others, and in China, two asymptomatic cases allegedly passing the virus to two others.
In all these studies, confirmation of ‘cases’ was made via PCR testing without regard to the possibility that any of the cases found might be false positives. The case numbers found, are in any event extremely small and certainly not sufficient to conclusively determine that asymptomatic transmission is a major component of spread.
It is also notable that, in what would seem to represent an abrupt volte face by the CCP, a further (presumably Government-approved) study from China was recently published which entirely contradicts the earlier conclusions regarding the phenomenon of asymptomatic transmission, which had been driven by Chinese data in particular, early in the pandemic.
Some might conclude that that study lacks the credibility one might expect for a paper published in Nature; it is claimed, for example, that they PCR-tested 92 per cent of Wuhan’s population (~10m individuals) over a 19-day period at the end of May, and found just 300 positive PCR tests, implying a false positive rate of no greater than 0.003 per cent. Further, it is claimed that while 100 per cent of the 300 PCR positive cases were asymptomatic, there were zero symptomatic PCR positive cases out of ~10m tested during a period only a few weeks after the epidemic had peaked in Wuhan.
If this seems incredible, then surely that has serious implications for the way in which earlier studies from China – data from which formed a significant part of the worldwide evidence base for asymptomatic transmission – should be regarded”.
These researchers have further submitted the following:
“Has the Evidence of Asymptomatic Spread of COVID-19 been Significantly Overstated?
Abstract
Evidence of transmission of SARS-CoV-2 from patients who remain asymptomatic (as opposed to pre-symptomatic) is found in a body of numerous meta-analyses. Evidence of asymptomatic transmission has been based on only a handful of instances which themselves are questionable. The existence of transmission of SARS-CoV-2 from asymptomatic individuals has become an accepted truth but the evidence for this phenomenon being anything other than mistaken interpretation of false positive test results is weak. Examination of the underlying data from the most frequently-cited such meta-analyses reveals that the conclusions are based on a surprisingly small number of cases (six in total globally) and, moreover, the possibility that they are all coincidental contacts with false positive results cannot be ruled out. Transmission which is pre-symptomatic is rare and represents a negligible risk to the population. It is questionable therefore whether any of the extensive testing, tracing, isolation and lockdown policies have delivered any worthwhile benefit over and above strategies which seek to advise symptomatic individuals to self-isolate.
Introduction
Many of the world’s economies have been seriously damaged on the basis of alleged evidence that people with no symptoms can spread SARS-CoV-2. It is essential that all such claimed evidence is carefully scrutinised because of the immense and ongoing impact of that claim on public policy making. Much of the early evidence of asymptomatic transmission came from China. Chinese publications appear to be major outliers in the scientific discussion and their contributions are, it is suggested, seriously distorting the available evidence in this area.
Scientific papers from reputable institutions which attempt to summarise the evidence have taken certain Chinese papers at face value. This has arguably resulted in the establishment of a dangerous assumption. The assumption is that there is compelling evidence that people who never have symptoms are capable of spreading SARS-CoV-2 to others.
This paper reviews the evidence that people who are asymptomatic (defined in this paper as not only having no symptoms but also never developing symptoms) are capable of carrying SARS-CoV-2 and infecting others. This must be clearly distinguished from pre-symptomatic – there is evidence that some patients can be infectious for a brief period before developing symptoms.
To the extent that pre-symptomatic cases exist the evidence suggests that they must only account for a very small proportion of transmission and therefore they present a low overall risk. In fact, in one study of 243 cases in total, the maximum transmission from pre-symptomatic individuals was estimated to account for less than 7%1 of transmissions. The secondary attack rate from pre-symptomatic transmission was estimated to be only 0.7% to household contacts in a large meta-analysis of 77,758 traced participants.2 Transmission which is pre-symptomatic is rare and represents a negligible risk to the population. The evidence that asymptomatic transmission exists at all is tissue thin. It is questionable therefore whether any of the extensive testing, tracing, isolation and lockdown policies have delivered any worthwhile benefit over and above strategies which seek to advise symptomatic individuals to self-isolate.
The evidence of transmission of SARS-CoV-2 comes largely from case reports where specific groups of infected individuals have been traced in an outbreak and the transmission routes are then reported. Deducing transmission from outbreak data is not straightforward and assumptions need to be made about which of the contacts caused transmission. This is not an exact science.
Reports of instances of transmission are important and interesting enough to publish but on their own they are merely anecdotal. Anecdotal evidence alone is no basis on which to formulate public policy. To draw conclusions about transmission it is necessary to gather multiple instances, ideally all, of such anecdotes and weigh them all up as evidence reaching a conclusion based on all the anecdotes together, i.e. in a formal meta-analysis. However, meta-analyses suffer from the flaw that they can be hugely skewed by larger data sets.
There have been numerous meta-analyses attempting to answer the question of whether SARS-CoV-2 can be spread by people who are asymptomatic. These have been published by distinguished scientists from a range of respected institutions. To reach a conclusion, the evidence from all the papers included in a meta-analysis is summarised. However, only by going back to the underlying data can we understand what the real risk of asymptomatic transmission is. We identified the most frequently-cited such published papers and examined the data underlying their conclusions. The bulk of the Chinese literature on asymptomatic spread were excluded by these meta-analyses because they did not meet the quality criteria specified by the authors.
Results
Across the studies reviewed, a total of seven instances suggestive of asymptomatic transmission were identified, these being:
In Italy, two asymptomatic cases allegedly passing the virus onto two others.
In Brunei, two asymptomatic cases allegedly passing the virus onto three others.
In China, two asymptomatic cases allegedly passing the virus onto two others
Notwithstanding the small numbers, these case reports, given undue prominence in papers written by respected authorities, appear to have played a major role in the evolution of lockdown and test and trace strategies adopted by most countries over the past nine months.
Findings from each of the four papers examined:
1. Yanes-Lane et al, from McGill University in Quebec,3 found 6,137 studies examining the issue of asymptomatic SARS-CoV-2 transmission and rejected all but 28 of them (due to small size, or inadequate methodology). Only 5 included reports of asymptomatic transmission and were listed in table 5 (figure1). As it happened, these were all reports of pre-symptomatic transmission. The study by Park et al. included four asymptomatic cases and four pre-symptomatic cases (hence these were listed separately in the table reproduced below) and there was no evidence of transmission from any of them.
Despite the only evidence of asymptomatic transmission (all of which were pre-symptomatic) being from China, an average was taken, concluding:
Among five transmission studies, 18 of 96 (18.8%) close contacts exposed to asymptomatic index patients were COVID-19 positive.
That sounds high until you consider that the sample size is just 13 index cases, all of which were pre-symptomatic cases, transmitting to 18 people across five studies, none of which were outside of China.
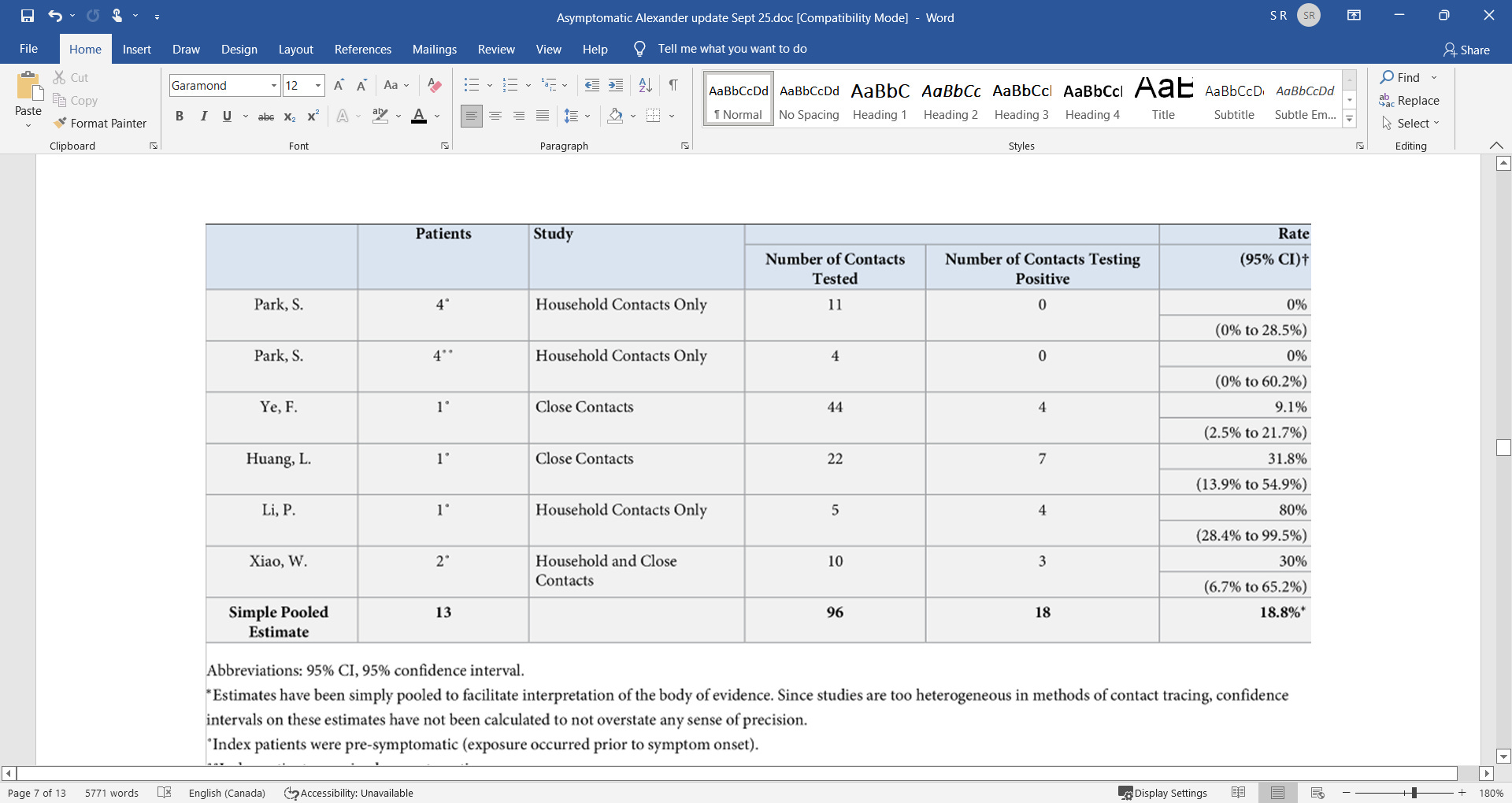
Figure 1: Table 5 of the Yanes-Lane et al paper. The two references to the study by Park et al. were from South Korea and the remainder from China
2. Buitrago-Garcia et al., from the University of Bern,4 found 688 studies on asymptomatic and pre-symptomatic COVID-19 and 5 which commented on transmission. Rather than draw conclusions on the likelihood of asymptomatic transmission they compared the risk from asymptomatic with that from symptomatic transmission. Included were three studies showing asymptomatic transmission, one from Brunei and two from China and two showing no transmission from Taiwan and South Korea.
As regards the Brunei study, which will be discussed further below, it is not clear how the numbers in this table were derived from the paper which reported on 71 patients and 1755 total contacts. Of these there were four instances of pre-symptomatic transmission and two incidences of true asymptomatic transmission, accounting for 11 and 3 cases respectively.
The two Chinese papers each only claimed a single patient had contracted COVID-19 from an asymptomatic person. Luo et al. studied 4950 people up until March 6th 2020 who were quarantined in Guangzhou.5 They had up to 6 PCR tests each with a mean of 2.4. From all this testing they only claim to have found eight asymptomatic individuals. They report on a single asymptomatic individual spreading SARS-CoV-2 but do not make it clear whether they were pre-symptomatic nor what symptoms the secondary case had. Nevertheless, this has been interpreted as evidence of asymptomatic spread.
Zhang et al.6 also reported from Guangzhou and two of the authors on this paper are the same as the Luo paper. Given the shared authorship, the possibility that this single case of probable pre-symptomatic transmission was the same individual reported in the Luo paper cannot be ruled out. This paper reported on the first 359 COVID-19 diagnoses and their 369 contacts up to 15th March 2020. Importantly, the single case of asymptomatic transmission was from a man to a male colleague who also remained asymptomatic (i.e. tested positive only, without symptoms). Given that the person said to have contracted COVID-19 had no symptoms this cannot be regarded as adequate evidence for transmission of disease.
Every test has a risk of producing an erroneous positive result, a false positive. A false positive rate of 1% would be very respectable for PCR testing and it is hard to find reports of false positives for PCR at lower rates than this. The UK Government’s own estimate for false positive results, based on other PCR tests for other viruses in non-pandemic situations is a median of 2.3% (range 0.8-4.0%),7 so a rate of 1% might be regarded as improbable given the speed of roll out of the test and other observations.
It is not clear how many of the people tested remained asymptomatic throughout, however, when testing 369 contacts a reasonable false positive rate of 1% would result in three to four false positive diagnoses. Given that all the contacts were tested because they had relationships with those that tested positive, any false positives found would by definition have been a contact with a case.
It is worth pointing out at this early stage that studies based on single figures such as this are no proper basis for policies affecting hundreds of millions of lives predicated on the questionable assumption that true asymptomatic transmission can regularly occur. It must be repeated that both studies so far contained a bare handful of alleged transmission without symptoms.
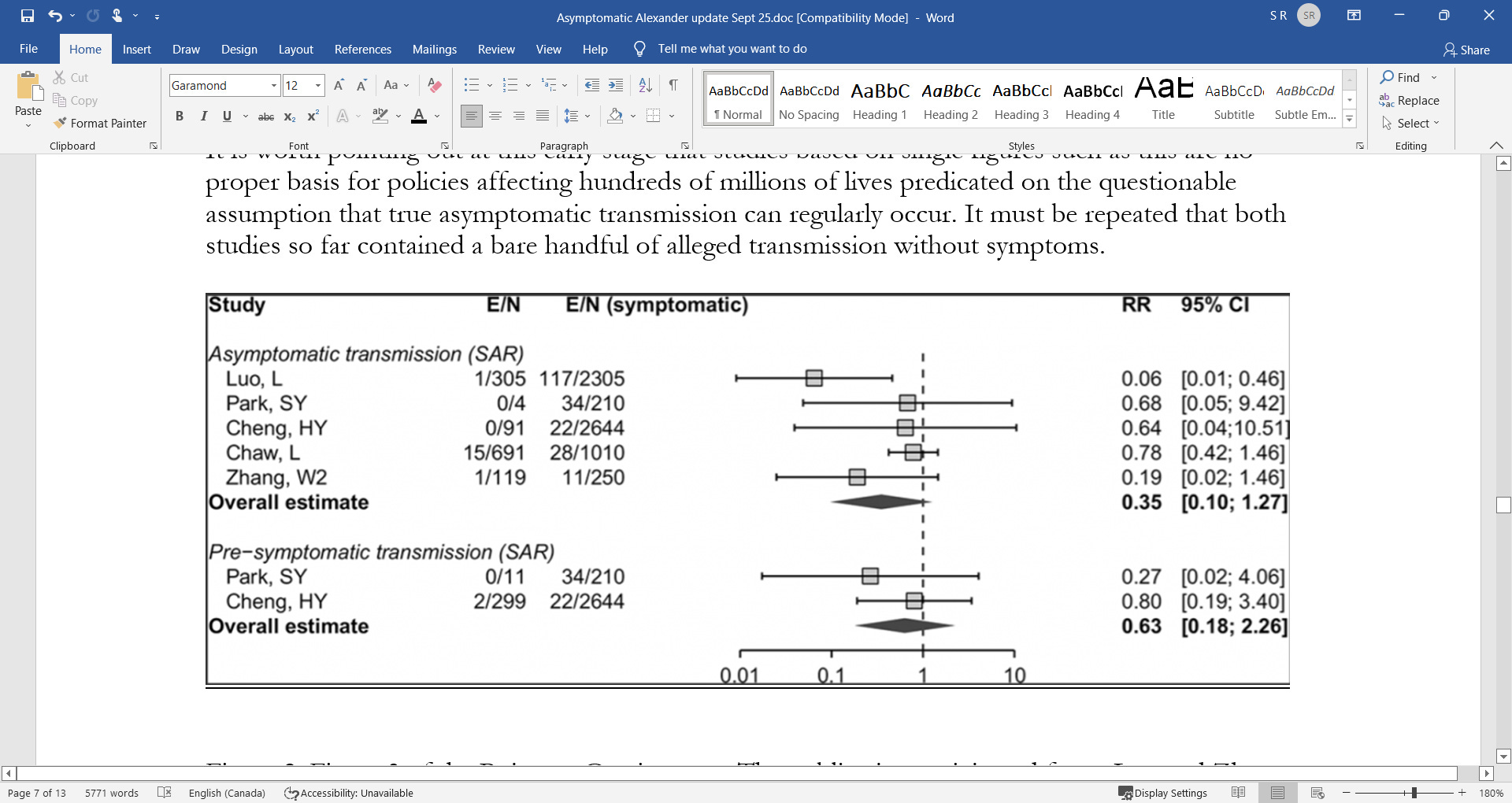
Figure 2: Figure 3 of the Buitrago-Garcia paper. The publications originated from: Luo and Zhang – China; Park – South Korea; Cheng – Taiwan; Chaw – Brunei. The first column shows the fraction of contacts contracting COVID-19 from an asymptomatic / pre-symptomatic individual and the second column shows the fraction contracting from symptomatic individuals in the same study.
3. Wee Chian Koh et al.8 also put great weight on the Brunei study but use different numbers for the same work. It is not clear why. No other cases of asymptomatic transmission were included in this analysis.
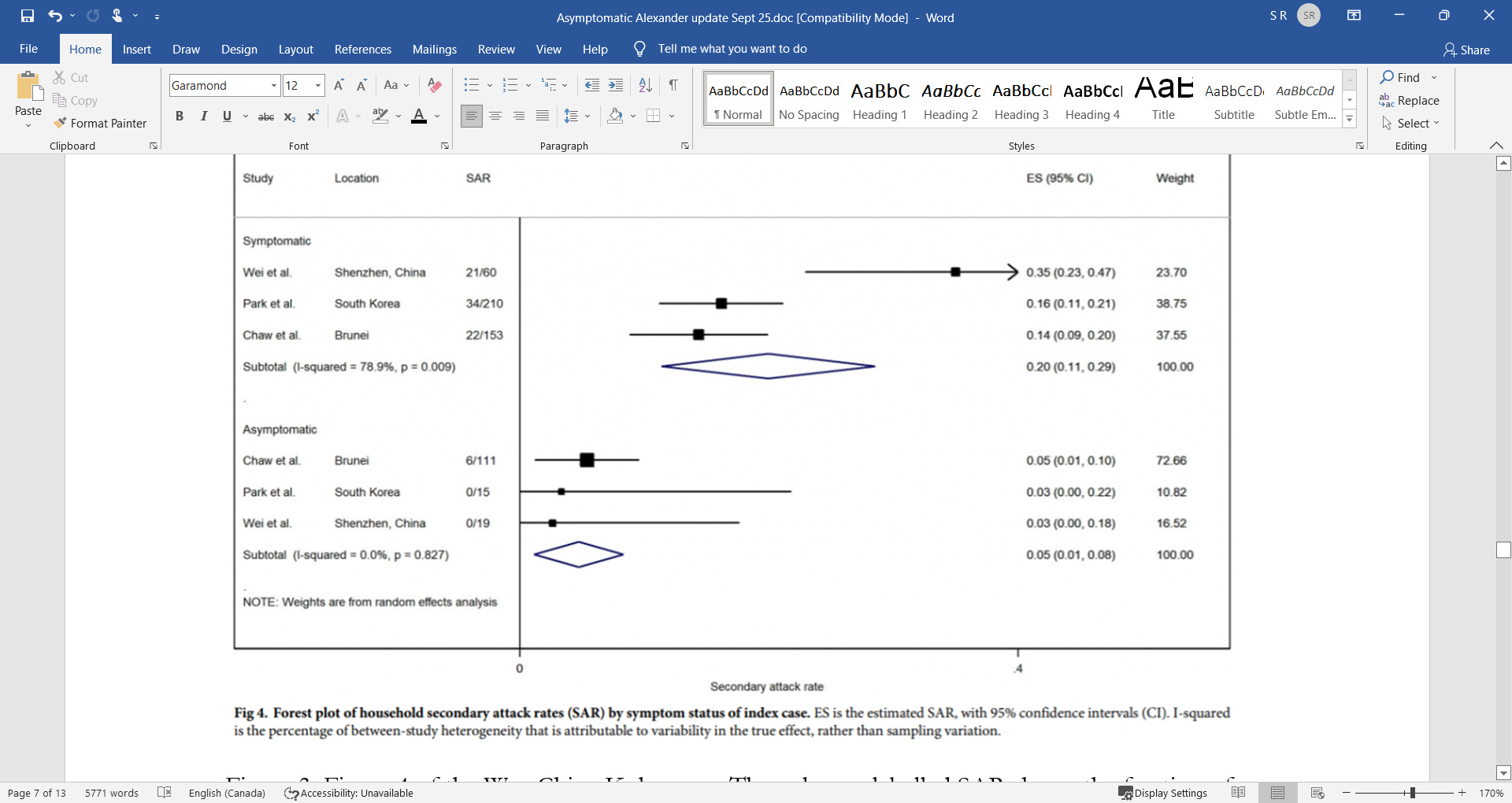
Figure 3: Figure 4 of the Wee Chian Koh paper. The columns labelled SAR shows the fraction of contacts that contracted COVID-19 in each study.
4. The Lancet pre-published a meta-analysis by Byambasuren et al.9 who found five studies from 571 met their minimum methodological criteria, two of which reported asymptomatic transmission. The first was a study of 4,950 contacts in Guangzhou5 who were quarantined.
The second study quoted was a Nature paper10 on an Italian study that did not actually report on asymptomatic transmission. Instead, they extrapolated from the results of PCR testing to deduce how much virus was present and assumed that high viral loads on testing equated to a higher risk of transmission.
The Italian study reports on numerous asymptomatic ‘cases’ and goes on to propose lines of ‘transmission’ concluding that two asymptomatic people were infected by two other asymptomatic people, out of 2,812 tested initially and then 2,343 tested again two weeks later. In the first round of testing, 29 of the 73 positives were asymptomatic. A respectable false positive rate for the testing performed would be 1%, therefore, it is reasonable to expect at least 28 false positive results when testing 2,812 people. It is therefore fair to conclude that all the 29 asymptomatic positives in the first round were most likely false positives.
In the second round of testing at the beginning of March, there were 18 asymptomatic people who tested positive out of 2,343 people tested. Likewise, these were most likely false positive results. Deducing chains of transmission based on a high risk of material numbers of false positive results is bad science.
Brunei study
Due to the prominence afforded to it by those justifying policy choices on the basis of asymptomatic transmission, it is worth focusing particularly on the study by Chaw et al.,11 from Brunei, which reported on a large outbreak which started with people who attended a religious festival and subsequently developed COVID-19. There were apparently six people who had no symptoms initially (of which, crucially for our purposes, two were asymptomatic throughout), but who allegedly spread SARS-CoV-2 from this outbreak to other people who did not attend.
There are two aspects of this paper that weaken this evidence:
Weak definition of a case (it appears any symptom of any severity was adequate)
High possibility of false positive test results
The same group published a further paper12 where they describe two of the incidences of asymptomatic spread in more detail. First there was a 13-year-old who attended the festival who is said to have spread SARS-CoV-2 to their teacher. The basis for this conclusion was that the teacher “had a mild cough for one day” along with a positive test.
The second was a father who remained asymptomatic but whose wife briefly had a runny nose and whose baby had a mild cough on one day.
In both these papers no details are given as to the testing protocols. A final paper13 reports on the first 135 cases to be diagnosed in Brunei. Thirteen of these first cases were asymptomatic. Without knowing the false positive rate of the testing and the numbers tested it is not possible to establish the significance of these asymptomatic ‘cases’.
Dr Chaw, the lead author of the Brunei transmission paper, was initially very helpful in correspondence with the authors. Thorough testing (with whole genome sequencing) was carried out for the first few cases but otherwise, as in the rest of the world, a positive PCR was considered sufficient. She was unaware (as are almost all doctors diagnosing COVID-19) of the criteria used in their laboratory to declare a test positive and has not responded to a request for further clarifications.
It is therefore at least arguable that the asymptomatic diagnoses in spring were all due to false positive test results. No testing system is perfect. Failure to acknowledge this and misinterpretation of positive results in patients with no symptoms has been hugely damaging. What is undoubtedly true is that the policy-making of governments responsible for the lives of billions of people around the world may in part be influenced by the dangerous assumption that there is persuasive evidence of asymptomatic transmission of SARS-CoV-2. It is far too soon to make that assumption and the evidence underpinning it is, at best, circumstantial.
Chinese Publications
During the early stages of the pandemic, many papers were published from China suggesting the frequency of asymptomatic transmission and its importance in SARS-CoV-2 spread. Notwithstanding that most of these were excluded by authors of the meta-analyses examined herein, their frequency, and the prominence afforded to these studies laid the foundations for this phenomenon being given undue salience in the scientific literature. This is despite asymptomatic transmission never having been a feature of previous respiratory pandemics and despite large studies showing no evidence of asymptomatic transmission outside of China. The reader will no doubt readily understand the challenges of relying heavily on the output of a highly controlled regime with an active interest in destabilising the economies and political systems of other countries.
It is notable in fact, that in what would seem to represent an abrupt volte face by the CCP, a further (presumably Government-approved) study from China was recently published14 which entirely contradicts the earlier conclusions regarding the phenomenon of asymptomatic transmission, which had been driven by Chinese data in particular, early in the pandemic.
Some might conclude that that study lacks the credibility one might expect for a paper published in Nature; it is claimed, for example, that they PCR tested 92% of Wuhan’s population (~10m individuals) over a 19-day period at the end of May, and found just 300 positive PCR tests, implying a false positive rate of no greater than 0.003%. Further, it is claimed that while 100% of the 300 PCR positive cases were asymptomatic, there were zero symptomatic PCR positive cases out of ~10m tested during a period only a few weeks after the epidemic had peaked in Wuhan.
If this seems incredible, then surely that has serious implications for the way in which earlier studies from China – data from which formed a significant part of the worldwide evidence base for asymptomatic transmission – should be regarded.
We do not claim to have included every meta-analysis that has been written on this subject, however the studies quoted here do represent the ones most frequently cited in support of the phenomenon of asymptomatic transmission. It is clear that these meta-analyses consist of highly questionable studies taken at face value.
What is an asymptomatic ‘case’?
Attempts to understand the phenomenon of asymptomatic COVID-19 have resulted in reports of asymptomatic cases accounting for between 4%15 and 76%16 of COVID-19 cases. An implausibly wide range such as this is evidence of an attempt to measure a phenomenon that is not a characteristic of the disease, in contrast to features such as symptoms.17
For completeness, it should be acknowledged that SARS-CoV-2 can be detected in asymptomatic people. They can test positive for SARS-CoV-2 virus and viable virus can be cultured from these individuals. In the past, this scenario of having virus onboard in the absence of symptoms would have been referred to as ‘immunity’ or else been attributed to a testing error. Someone with immunity cannot prevent virus entering their respiratory tract, however, when that occurs, their immune system invariably deals with the attack and they remain oblivious and have no symptoms.
It is for the above reasons that whereas reports of high numbers of asymptomatic cases, for example in cruise ship outbreaks,18 are cited as evidence of asymptomatic transmission, we contend that a more plausible explanation for most of these observations is in fact prior immunity. Several prominent papers made unsupported claims of asymptomatic transmission simply because they had found asymptomatic individuals who had tested positive during an outbreak.19 Asymptomatic transmission can only be proven by clear evidence that a patient has been infected by SARS-CoV-2 from a person who was asymptomatic. Finding positive test results in asymptomatic individuals is not evidence of transmission.
Normally, someone who is immune would not be considered to have a disease or to be a ‘case’ in an epidemic. It is only in the current crisis that mass testing of asymptomatic individuals has resulted in the detection of virus in asymptomatic individuals. Considerable further work would be required before it could be confidently stated that asymptomatic positives could ever transmit infection.
There is certainly no evidence of immune individuals (as historically defined) transmitting other respiratory viruses. Viral replication and shedding20 is a prerequisite for viral spread and in immune individuals virus is prevented from growing exponentially so the viral numbers remain low. Attempts to deduce viral numbers present from the quality of the test results (viral load on PCR) is overinterpretation. However, no assumptions have been made here. The evidence as to whether immune individuals can transmit SARS-CoV-2 virus must come from actual studies that show, or do not show, real world transmission.
Aside from reported studies of transmission, those leading on the contact tracing response might have useful experience on the likelihood of transmission. Maria Van Kerkhove, head of the World Health Organization’s emerging diseases and zoonosis unit21 stated at the beginning of June:
Countries doing very detailed contact tracing …[are]…following asymptomatic cases and following contacts and they’re not finding secondary transmission onwards. It’s very rare. Much of that is not published in the literature.
It is worth noting that an early frequently-cited claim22 of pre-symptomatic transmission has been discredited23 after it was revealed that the authors did not interview the patient accused of spreading infection who was in fact symptomatic at the time of transmission. This has not been retracted.
Conclusion
Medical evidence can be difficult to summarise. The medical literature is huge and constantly growing and it is impossible to say with confidence that everything of relevance has been read. This in itself can cause problems: it is difficult to say confidently that there is zero evidence for something. That is why this paper has been careful only to claim that it is a dangerous assumption to believe that there is persuasive, scientific evidence of asymptomatic transmission.
It could be argued that adherence to ‘precautionary principle’ demands that public policy assumes the existence of significant asymptomatic transmission, in order to be ‘better safe than sorry’. However, given the increasing evidence of the harms caused by such policy, at some point the burden of proof must surely shift onto those advocating extreme measures. There is increasing evidence of harm from interventions, for example: there are over 100 excess deaths at home per day in England; accident and emergency attendances are well below normal levels; excess mortality in the under 60s is significant; prescriptions for heart medications are well below normal and there are excess deaths resulting from heart disease.
The Chinese Communist Party24 has mandated that all scientific literature on COVID-19 must first be approved by the Chinese Ministry of Science and Technology or Ministry of Education before publication. This political interference means that all Chinese scientific publications should be regarded as suspect.
Additionally, there is an unknown but real risk of publication bias because studies, such as the many early Chinese ones showing asymptomatic transmission may find a quicker route to publication, whereas an article reporting the opposite may risk not having commensurate perceived salience when the editors of a journal are choosing papers for publication. It is important to note that much of the evidence relating to modes of transmission was shared via pre-prints prior to publication, and decisions had to be taken based on evidence that had not been peer reviewed, as is inevitable in a pandemic situation.
A claim is not being made that every meta-analysis has been included here and this article may be updated in due course with more data as it becomes available.
However, after examination of the most frequently-cited papers in this area available to date, we are struck by the paucity of persuasive evidence of anything but the most minor of symptoms resulting from supposed asymptomatic spread; most or all of which could be misdiagnoses and in any event are at no more than anecdotal level. There is no evidence, outside of China, that anyone has developed even moderate COVID-19 based on true asymptomatic spread, as opposed to pre-symptomatic spread”.
Source – https://palexander.substack.com/p/asymptomatic-transmission-was-a-lie