
Pierre Kory, MD, MPAMay 16
In part I of my post on the TOGETHER trial of ivermectin, I presented the context of this trial within Big Pharma’s decades-long Disinformation campaign against “science inconvenient to their interests.” I argued that no science has ever been a greater threat to Pharma than the massive efficacy data of the generic drug ivermectin in COVID-19. I detailed how they have long deployed “studies designed or conducted to fail” and/or “studies manipulated to show positive results.” They do both. Repeatedly. They then publish these studies in a small number of captured high-impact scientific journals which influence the captured media and then are recommended for or against by captured health agencies.
Note that the importance of the wording of the conclusion in a trial’s abstract, published in a high-impact journal, cannot be overstated. Only a small minority of physicians read and think critically about the full study manuscript. Even less read the full study abstract. Sadly, the overwhelming majority simply read the abstract’s conclusion. In this manner, and particularly in the case of the TOGETHER trial, they can baselessly and erroneously convince the vast majority of doctors and citizens that ivermectin is ineffective. In the case of ivermectin, they did this via less than a handful of severely flawed “Big RCT’s” despite the overwhelming mountain of valid OCT’s and RCT’s and the success of health ministry program success in COVID. The TOGETHER trial on ivermectin was never going to be a positive trial. Ever. That was a foregone conclusion.
So what I want to do here is break down exactly how they accomplished this feat, using the most brazenly fraudulent conduct of any trial I have studied. This is NOT to say that I have never witnessed fraudulent studies, but this trial displays an unprecedented number of targeted tactics designed to deny, suppress, and distort the evidence of efficacy.
First off, this trial was designed and conducted by researchers employed by companies with deep ties to Big Pharma (Pfizer specifically) and/or the Bill and Melinda Gates Foundation (BMGF). Recall the latter essentially defends and represents the intellectual property rights and goals of the entire vaccination industry). The Pharma associations by study investigators are so common that it association is not automatically an indictment (but should be).
Please realize that the numerous connections to Pfizer are particularly troubling here. Pfizer’s Paxlovid is a direct competitor to ivermectin. Paxlovid stands to make many tens of billions of dollars around the world with no upper limit as the pandemic promises to rage on. Paxlovid is composed of a formulation with a single mechanism shared with ivermectin. Yet, somehow it has important drug interactions with almost every class of medicine known. Ivermectin on the other hand, has many more anti-viral and anti-inflammatory mechanisms, yet has almost no drug interactions. It is one of, if not the safest and most inexpensive and widely available medicines in history. Just sayin’. Note that one TOGETHER trial investigator, Craig Rayner, works for a company that works for Pfizer. What is fascinating is that he published the world’s first “anti-ivermectin” letter way back in June of 2020 after the landmark Monash University in-vitro study found that ivermectin eradicated SARS-CoV2 in a cell culture model. Note that he did so.. before a single clinical trial had been done in COVID. Interesting no? Probably just a coincidence.
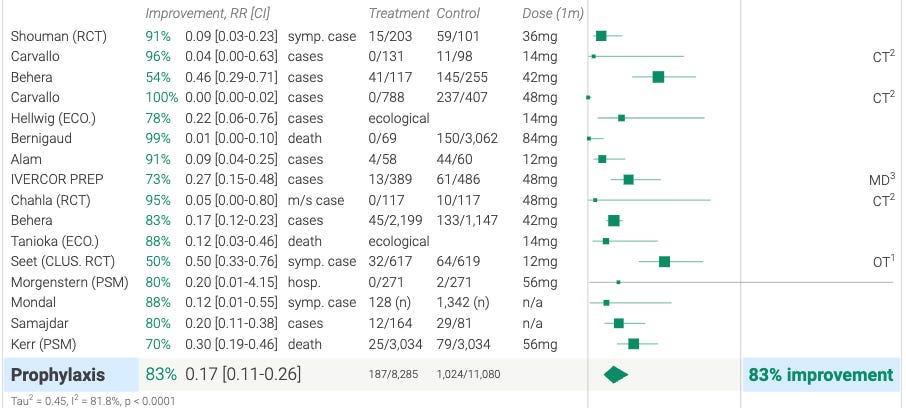
Further, the over a dozen markedly positive trials supporting ivermectin in prevention against COVID-19 make the drug a direct competitor to the vaccines. The 65+ trials showing efficacy in treatment would remove the EUA for the vaccines (if “science” was functioning). Thus, ivermectin is a direct threat to the entire COVID-19 vaccine industry as well. So, to be clear, ivermectin has the largest Big Pharma market forces arrayed against it than any other generic medicine in history. The below chart summarizes the prevention trials (which include multiple RCT’s forthose of you who are RCT fundamentalist church members). This impressive chart is why the captured WHO, in their last guideline document on ivermectin, simply stated, “we did not review trials of ivermectin in the prevention of COVID-19.” How convenient. This is also a new “play” in the Disinformation playbook which I will call “The Ignore.” When inconvenient science like the below pops up, just ignore it.
Beyond the many concerns I myself identified in the TOGETHER trial and among its investigators, this post also relies on the work of a large network of colleagues and experts. They uncovered even more concerning flaws than I would have been able to do alone. I find their work unparalleled in meticulousness, depth and importance. At the top of those doing “deep dives” (please visit their linked Substacks) are the polymaths Alexandros Marinos and Phil Harper, but the list also includes PhD’s in statistics (David Wiseman) and epidemiology (Harvey Risch), and expert clinicians or researchers (Flavio Cadegiani, Jackie Stone, David Scheim) among others. Also at the top is the expert scientist group c19early.com, as they have the most comprehensive (yet far more concise) list of identified issues here. Reading their take on the trial is shocking, yet their conclusion is too mild for what they found, i.e. “these results are unreliable.” Read their more concise explanations of the 47, yes 47, major concerns, with many being what I call “fatal flaws.” I will go through quite a few of them below before I will stop with exhaustion and disgust. Here is the list from ivmmeta.com:
Many major issues including multiple impossible numbers, blinding failure, randomization failure, and many protocol violations, as detailed below
Protocol issues: blinding failure unequal randomization, significant confounding unknown onset patients included widespread community use DSMC not independent extreme conflicts of interest vaccine inclusion changes analysis company works closely with Pfizer designed by Cytel Δ viral load not reported per-protocol conflict vs. fluvoxamine multiple conflicting randomization protocols conflicting dosing plasma concentration below known effective primary outcome easy to game conflicting target enrollment futility threshold inconsistent subgroup analysis missing analysis missing outcomes mid-trial protocol changes imputation protocol violation single-dose recruiting continued after change funding list incorrect SAP after trial start single dose results not reported placebo unspecified
Data issues: unexplained delay no response to data request 3 different death counts patient count mismatch conflicting placebo arm counts unknown onset results dramatically better low active arm side-effects incorrect conclusion conflicting comorbidity counts conflicting adverse event counts screening to treatment delay missing age information mean delay likely excluding unknown onset two different per-protocol counts 3-dose placebo much more effective dominated by Gamma variant, no discussion
The deep Big Pharma/BMGF ties of the main study investigators are not a barrier to publication in Big Journals (if anything they’re a boon). However, many of the other flaws are so profound that, if sanity and ethics reigned, the study would never (should never?) have been accepted by a major journal. But lets go anyway:
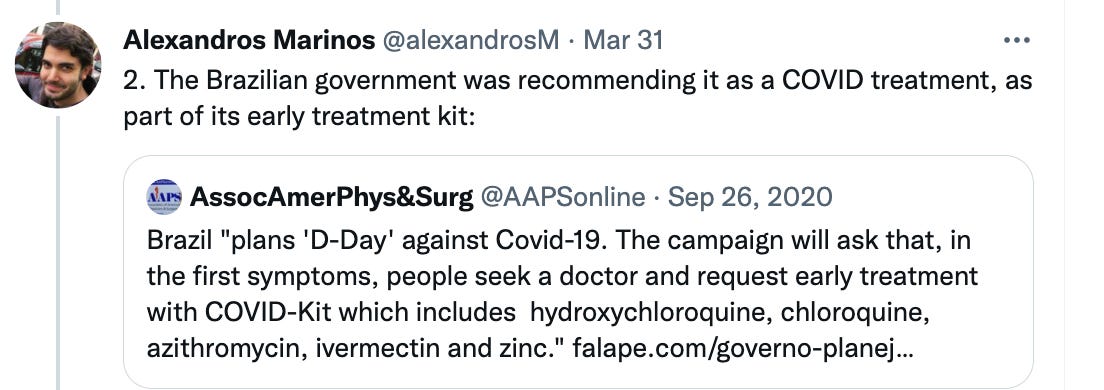
- The investigators knowingly conducted the trial in an area where ivermectin use was rampant, yet they did not explicitly exclude patients taking ivermectin from the control group. This was done despite all the other ivermectin trials having had this as an exclusion criteria. Excluding patients already on a medicine from an RCT that is studying the medicine is Research Trial Design 101. Solely on this basis, this study should have been dead in the water upon arrival to NEJM. Fraud or incompetence? You choose. That same question should also apply to all issues following. One investigators defense was “but we carefully screened for ivermectin use.” I am sure you did, but please explain why it was not made an explicit exclusion criteria? Indefensible. Full stop. Again, not subtle folks. The biggest “tell” of fraud. I mean, how can you show efficacy when both groups have access to the same drug? Palm to forehead. See below from Alexandro Marinos’s brilliant thread on this topic:


To paraphrase Alexandro’s words, we really do not have to go farther to call foul on this trial. It’s what is called a fatal flaw (or fatal fraud). The consequence of not specifically and primarily identifying people on ivermectin is that they run the welcome risk of comparing those taking ivermectin… with many/most/all in the control group who were also taking ivermectin. It is hard to prove that a medicine is better than itself. It’s almost as if they wanted the control group to take ivermectin. But here’s the thing, they don’t need everyone in the control group to be on ivermectin in order to bury the efficacy signal, they only need enough to.. avoid a statistically significant benefit. Mission accomplished. Indeed, the reality of this trial is that, in the duplicitous words of the Principal Investigator Ed Mills, “I don’t understand the psychology of the ivermectin advocates. They fail to see the positive in this study and just focus on it not being overwhelmingly positive. I actually think it is quite positive.” Yet while he said this privately, what he said to the newspapers was ,“there was no indication that ivermectin is clinically useful.” He wrote the conclusion as “treatment with ivermectin did not result in a lower incidence of medical admission to a hospital due to progression of Covid-19.” Yet, buried in the supplementary appendix is the result of a complex statistical method (Bayesian analysis), which most statisticians consider to be the most robust at determining efficacy. That analysis found a 79.4% probability of the superiority of ivermectin. Shocking I know.
Then, beyond conducting a trial of ivermectin in an area rife with use of a government recommended, widely available, over-the-counter (OTC) medicine while not having a clear exclusion criteria for use, it gets flagrantly worse (if that’s possible). The placebo tablets were not identical to the ivermectin tablets. Bottles yes, tablets no. There was only one manufacturer of ivermectin in Brazil at the start of the trial, you could buy the brand everywhere OTC, yet matching placebo tablets were not produced. Note they used tablets instead of capsules. To explain, active medicine and placebo capsules can be made to look identical to each other very easily (just a different powder inside) whereas tablets cannot unless the ivermectin tablet manufacturer makes the same tablet but without ivermectin. They chose to use publicly recognizable tablets while the placebo group got tablets that did not look like Brazilian ivermectin. Don’t you think that every trial participant was dying to know whether they got the real stuff or the placebo? Research Design 101, once again. Incompetence or fraud?
More evidence that the placebo group took ivermectin is in the manuscript, which reported less gastrointestinal side effects in the ivermectin arm. For comparison, there was a 3.6 times greater incidence of diarrhea in the ivermectin treatment arm in the recent media misreported Malaysia trial. This finding also reminds me of the first Pharma bomb dropped on ivermectin, published in the high-impact journal Clinical Infectious Disease, where they found largely equal rates of common ivermectin side effects in the placebo group such as blurry vision and diarrhea. That study was done in Colombia, another country where ivermectin use was rampant during a time of massive fear-mongering and death. Anyone want to be the placebo in the midst of a catastrophic threat to your life?
The next issue, for me personally, betrays fraudulent intent like no other. That is the repeated, aggressive, and overt attempts to limit the dose and duration of ivermectin. The reason why this is as telling of fraud as the above, is that this tactic has long been Pharma’s main, time-honored approach when trying to disprove generic treatments (like Vitamin D or Vitamin C). They conduct a trial using either too low of a dose, for too short a duration, or at the wrong time-point in the disease. But here’s the deal. They do not have to be subtle. They just have to get it published in a high-impact journal and the headlines get written. Since the NEJM was such a wide-open non-gate keeper for all these flaws, err, I mean frauds, they sailed through to publication. But check out these insanely obvious, patented, dosing shenanigans:
- They started the trial with the ivermectin arm getting a single dose only, at a time when almost all treating clinicians around the world, including the FLCCC, were using multi-day regimens, and would treat up to 5 days or until recovered. One investigator tried to defend this by stating that they adopted the same dosing approach as with parasites. Yet, in their introduction, they report on the the ten years of anti-viral activity found among in-vitro studies as explored in our (and others) review paper.
- They then increased the duration of treatment, after it started to dawn on them that they couldn’t “disprove” or “prove” anything using an incredulous single dose. But, get this, they then only extended the duration to 3 days. Again, no other anti-viral is used for 3 days – Molnupiravir and Paxlovid are 5 days (with the Boston Globe now reporting that patients are falling ill again after stopping Paxlovid, with the CEO of Pfizer flippantly saying, “just take a second course.” Acyclovir (7-10 days), Tamiflu (minimum 5 days), Ganciclovir (7-10 days). So why just 3 days against a deadly virus with one of the safest drugs known? Further, the senior author has given contradictory statements as to how they chose the dose. He wrote it was based on “feedback from advocacy groups.” I happen to know it was done due to pressure from one of the funding organizations of the trial who called foul on the one-day dose gimmick. Calling them “an advocacy group” is an insult. If he means the FLCCC is the “advocacy group”, I can vouch that we never talked to any investigator before they made that change. But in an email reply to someone who asked about the dosing, The Principal Investigator wrote a bunch of lies about how he proudly collaborated with me and the FLCCC to arrive at the dose. Bullshit. I will go into this nonsense in more detail in Post 3 of this farce of a trial where I will compile all the duplicitous, false, and sinister statements by these investigators.
- The other most blatant dosing shenanigan is when they attached an unprecedented and inexplicable “weight limit” of 60kg to the initial 0.4mg/kg single dose protocol – meaning the more you weighed over 60kg (the equivalent of only 132 lbs!) you smaller dose you would get per body weight. It’s not like they knew the obese fare worse in COVID or anything, right? Also, where the hell is this weight limit from? Totally invented. When treating parasites, there is NO weight limit. None. Ivermectin distributes to fat tissues. You need to dose to actual body weight. The investigators even foolishly cited studies using single doses up to 800 mcg/kg as being safe in their ethics approval application.
- They then apparently had second thoughts on this low, ridiculous, and arbitrary weight limit of 60 kg because when they changed the protocol to 3 days only, they reset this novel limiting of weight to a 90 kg limit (still only 198 lbs). Problem: 50% of people in the trial had a BMI over 30, thus the majority of these patients got an even lower dose per body weight. They did whatever they could to give as little as possible. Not subtle. Also, our Brazilian colleagues battling the extremely high viral loads of gamma were using 0.6-1.0mg/kg which is roughly DOUBLEtheir dose, for TEN days, which is roughly TRIPLE their dose. Further, the “real doctors” on the ground in Brazil during gamma, amidst the dying and deteriorating, were combining ivermectin with nitazoxanide (an equally effective repurposed anti-parasite drug) and other anti-inflammatory and/or anti-androgen therapies. Talk to Dr. Flavio Cadegiani, a doctor who actually figured out how to treat the gamma variant. Wait, I’m sorry, doctors don’t know what they are doing anymore, it is the big captured federal agencies, full of Gods of Science and Knowledge whom we should be listening to. Sorry Flavio.
- It gets worse folks. They also recommended that subjects take their dose on an empty stomach, knowing full well that concentrations would be higher if taken with a full stomach. What is even more disturbing about this recommendation is that one of the more Pfizer-conflicted investigators of the trial, Craig Rayner, published the first “anti-ivermectin” Letter to the Editor for COVID-19 in June of 2020, as I mentioned previously. I repeat. In June of 2020. He was the world’s first published ivermectin naysayer. Again, before any clinical trials had even been done in COVID. I suspect Pfizer must have really wanted to get ahead of any enthusiasm for ivermectin. The letter attempted to mitigate the excited global response and media fanfare that erupted after the publication of the highly positive in-vitro ivermectin SARS-Co-V2 experiment by Caly and Wagstaff from Australia’s Monash University. Rayner knew higher concentrations could be achieved because in that letter he writes “Merck’s product information reports that administration of 30mg ivermectin following a highfat meal resulted in an approximate 2.5-fold increase in bioavailability relative to administration of 30mg ivermectin in the fasted state.” What is hilarious is that he did not know then that he would be part of a trial which stipulates that subjects take the drug.. on an empty stomach.
Note Rayner’s letter literally invented the first anti-ivermectin narrative that “standard dosing in humans could never reach effective blood level concentrations required in the in-vitro monkey kidney cell model.” We in the FLCCC fought that one for many months. Please note, doses used in-vitro often bear little resemblance to human dosing, yet this narrative was hammered for many months through media and academia. Read this excellent post from Joomi where she explores how erroneous such reasoning and claims are. My favorite is this quote:
Ivermectin’s mode of action against parasites in the human body remains to be clarified. There is a substantial disparity between maximum plasma concentrations after ivermectin administration and the concentrations needed to induce paralysis in microfilariae.
This “impossible dosing” narrative was then joined by others like “it only works in places with endemic parasites/worms” and “all the positive trials are too small or too low quality to rely on” and “many trials were suspected to be fraudulent.” Let’s not forget about the hurtful and insulting narratives targeting clinicians and researchers trying to bring evidence of efficacy to the masses (Paul Marik, myself, and the FLCCC). Insinuations that we should not be taken seriously, how we have a “religious” belief in ivermectin, or how we are simply an “advocacy group” instead of a highly published group of experts and researchers with decades of experience and deep expertise in many aspects of COVID. The biggest gun in those attacks was the Big Pharma rag called MedpageToday.com which published numerous derogatory headlines and articles with insulting quotes by physicians no-one has ever heard of. Sorry for I digress.
Building these narratives is a critical tactic in their global Disinformation campaign. These propagandized “narratives” have been parroted to the press by several of the TOGETHER trial authors to the press. This interview with ED Mills, the senior author of the TOGETHER trial is full of them. The NEJM TOGETHER trial manuscript even includes a paragraph of propaganda narrative right in the introduction, for all the zombie, read-the-abstract only doctors:
More than 60 randomized trials of ivermectin for the treatment of Covid-19 have been registered, and findings have been reported for as many as 31 clinical trials. The results have been discordant, and various review groups interpret the evidence differently — some advocating for benefits of ivermectin, and others reticent to conclude a benefit. However, most trials have been small, and several have been withdrawn from publication owing to concerns about credibility.
Now check out the stuff spewing out of this Ivory Tower Canadian researcher below. This is what a victim of medical journal and mass media propaganda will say (taken from a review by the excellent ivermectin researcher Mikka Turkia):
“Canada research chair in Health Law and Policy at the University of Alberta wrote about ’why the Covid cult of ivermectin won’t die … the debate over its use is really about ideology and in-group signaling — not science … one of the most nonsensical storylines in a sea of nonsensical storylines . . . the ivermectin bunkum continues . . . there have been several recent large, well-done, clinical trials, including one published in the New England Journal of Medicine on Wednesday, that definitively show, according to one of the study’s authors, “there’s really no sign of any benefit.” The author mentioned demands for retraction, smuggling ivermectin into hospitals inside teddy bears, legal cases demanding administration of ivermectin for inpatients, and the use of ivermectin to treat parasites in horses (this part is actually all true and I am fiercely admiring of all those who did what they knew their loved one needed) . He wrote that research had shown that people who believed this kind of misinformation were ‘less likely to adopt preventive strategies, such as wearing masks, physical distancing and, of course, getting Covid vaccinations’, adding that ’the ivermectin believers never really address the conceptual inconsistency of why it makes sense to advocate for an unproven pharmaceutical treatment with known side effects over a vaccine that has a mountain of evidence demonstrating efficacy and safety’. He concluded that ’a vaccine that is given free by the government for the benefit of the entire community smells like socialism, I guess. While taking an unproven therapy is something individuals do for themselves. Freedom!’ Astonishing display of the wicked power of propaganda. Wow.
OK, back to this damn trial. Another action they took was allowing subjects to enter the trial.. up to 7 days from symptom onset, and then allowed another day to get randomized and medicine delivered. And then it gets even worse – they didn’t exclude from analysis the subjects who needed hospital within 24 hours like they did in the other arms of this trial. Why have a different approach in the ivermectin arm? Weird no? Note that by doing this, they hurt only the ivermectin arm. Placebo patients were going to go to the hospital anyway.. because they got placebo and it was not going to change their trajectory. Ivermectin, if it worked and was going to change the trajectory of a patient away from the hospital, would need at least a day to do so. But no, in this arm of the trial, with this particular medicine, they removed the 24 hour exclusion period where the hospitalization would no longer be counted. Thus, by doing this, you can selectively increase the number of hospitalizations that counted in the ivermectin arm. Clever no?
Remember, ivermectin is an anti-viral. Anti-virals work best in the first days of symptoms. The trial was held during the rapidly sickening gamma variant where some patients were entering hospital within 3 days of symptoms. Here, you could start treatment up to 8 days from first falling ill, and if you landed in the hospital within 24 hours.. it counted. Brilliant. Note how in the Paxlovid trial their cutoff was that treatment had to begin within 3 days of symptoms. It’s nice to be Big Pharma where you know how to design a trial when you want to show something works (and you know how to design a trial when you want to show something supposedly doesn’t work).
So, time from first symptoms within 7 days was an inclusion criteria. Yet in the manuscript, they are missing the “time from symptoms” for a whopping 317 patients. How can you know whether to include a patient in the trial if you don’t know the time from first symptoms? How can this data be missing? It gets worse. Guess how well the ivermectin group with missing data did? By “reverse” calculating, David Wiseman found a statistically significant reduction in need for hospital of 49% among those missing patients. Yup.
Have you had enough yet or should we we keep going? Fine, lets push on but if you want to take a break I will understand as this gets tedious and infuriating at the same time because you are literally watching a mass murder unfold.
Now, they knowingly conducted the trial in a country that is the single largest buyer of pharmaceutical products in the world. This is because Brazil has the world’s largest national health system and it buys all of its medicines en masse. Do you think that might invite corruption around the pharmaceutical industry? Unsurprisingly, the contract research organizations (CRO’s) that conduct pharmaceutical research trials in Brazil are also notoriously corrupt and/or corruptible. To wit, in the multi-country trial of Merck’s molnupiravir, it was found to be effective in only one country. Guess which country? BRAZIL! The CRO that conducted this trial is headed by the first author. His CRO has long conducted only Big Pharma trials, never having done one on any generic drug. At minimum, one can ponder what his future opportunities for Pharma contracts would be like if he killed the industry with a positive ivermecitn study. Ugh.
Next, the complex design and opaque manner in which they assigned patients to different medicines and different placebos made it very difficult to identify the egregious nature of this next action. We only know it due to the incredible work of Alexandros Marinos, Phil Harper, and the expert scientist group c19early.com.
From Alex Marino’s deep dive, he found that they could not have enrolled ivermectin and placebo patients at the same time, as they claim they did. In fact, the ivermectin group was enrolled far, far more frequently at the beginning and during the gamma surge, a variant 4 times as deadly as the others. There was no way this should have ever happened, and it contradicts the manuscript and their public statements. The investigators repeatedly stated that they enrolled patients to the various medicines and placebos equally and concurrently, in what is called a 1:1:1:1 ratio. Fluvoxamine and ivermectin and their placebo arms ran concurrently. Yet, suddenly, as death rates started to climb due to gamma, they started to enroll far more patients into the ivermectin treatment arm than fluvoxamine or any other placebo arm. Hmm. Just bad luck for ivermectin I guess.
Next, for unclear reasons, the 3-day, fully compliant placebo group of the ivermectin arm of the trial outperformed the other placebo groups of the other medicines enrolled in this trial. Stroke of bad luck for ivermectin or a cherry-picked placebo group? This is insane.
The last two issues are only possible because of this largely novel trial design with so many different placebo groups – i.e. there were 1,3,10,14 day duration placebo groups assigned to different study medicines at overlapping times. This type of complicated trial, in my mind, literally created a screen for them to manipulate which patients they wanted to compare. Not saying they did (fuck it, maybe I am), but it is damn curious how the best performing placebo group of all the medicines studied.. was the ivermectin-specific placebo group. Oh yeah, I know why, it’s because that placebo group was not excluded from taking ivermectin. Whoops, I forgot.
Another curiosity is that the findings of this trial differed markedly from a larger Brazilian study done by researchers devoid of pharmaceutical company financial ties (Lucy Kerr, Flavio Cadegiani et al). In that study, they meticulously analyzed the prospectively compiled data by the city of Itajai as it conducted a city-wide prevention program with ivermectin which included 159,000 inhabitants. Among the 113,000 that took ivermectin regularly, massive reductions in cases (-49%), hospitalizations (-68%), and death (-70%) were recorded. Note that was a study of using ivermectin only in prevention. The small minority of Itajai’s inhabitants who did go to hospital were not treated with ivermectin. Thus that massive study shows the bare minimum of the true effectiveness of ivermectin if used in both prevention and treatment. Min-i-mum.
The inarguable reality is that ivermectin is a wickedly effective drug in COVID. Yet, the TOGETHER trial, using a hyper-complex, multi-concurrent, multi-arm trial fraught with a willful inability to truly blind the study, successfully managed to conclude it is not effective. Go figure. I maintain that the complexity and non-transparency of the trial made it a perfect vehicle for these Pharma-conflicted investigators to commit fraud. But let’s say there was no fraudulent intent. Then I would maintain that due to the 47 major concerns identified by the c19early.com group above, this was the most incompetent and sloppily conducted trial ever. Enough with that. This atrocity was a screaming fraud. If they want to plead incompetence it would be tough. The main investigators are from some of the top research institutions in the world and they literally call themselves “trialists,” given they do this for a profession. They have one job. Design and conduct a good, clean trial because the fucking world depends on it. Do a trial like Dr. Flavio Cadegiani’s proxalutamide trial, the highest-quality graded large trial done in the pandemic to date. That trial found a statistically significant, massive mortality benefit of an $11 medicine. The British Medical Journal has been sitting on his study for almost a year now, refusing to publish or reject it to date. I am not making this up.
This trial should be called out as a fraud by the wider scientific community, not just me and the several dozen top researchers I have the honor to work alongside. Many of these colleagues have been relentlessly attacked and discredited for trying to bring out various truths. Again, this “Diversion” tactic is not new. See my “addendum” below which contains a review of the same tactics pulled with regard to suppressing the efficacy of Vitamin D over decades. That review was compiled by Dr. William Grant, one of the world experts in Vitamin D. Pharma HATES vitamins. Dr. Grant recognized that Pharma was pulling the same stuff in COVID in regards to ivermectin that he had witnessed during his career in regards to Vitamin D. So, in early 2021, he sent me “the Disinformation Playbook” article from the Union of Concerned Scientists, warning me what was going on. I received that email at a time of my life and that of the FLCCC that was going sideways fast. I/we just could not understand what the hell was going on. We had identified a solution to the pandemic and not only was no-one listening, they were attacking our findings, our paper, and our credibility. Then I read that article and..Everything. Started. To. Make. Sense.
Again, what I find hilarious is that despite these maneuvers they still reported reductions in hospitalizations and mortality. Most of my colleagues feel the size of the reductions have been purposely misrepresented or even fabricated to ensure a finding that was not “statistically significant.” Their critique of this trial will be made public soon, but the most damning “tell” of fraud is that the study investigators, in their original study protocol, stated that “the individual patient level data (IPL)” will be publicly available at the completion of the protocol. I cannot emphasize the critical importance of study data transparency and availability. This is what the FLCCC’s Flavio Cadegiani has done with all his trials data. Immediate and public availability of IPL data. He then responds to all concerns, critiques, and queries from the public with thoughtful and clarifying responses. His intelligence, efforts, integrity and courage throughout the pandemic has been unparalleled. The attack on him by the BMJ was astounding in its falsity and depravity. Good guys can’t win apparently.
This public data transparency (which Pharma trials now apparently only do under court order) is also what Tess Lawrie and the World Council for Health have long recognized as one of the most important requirements to restore integrity to the scientific process. With the TOGETHER trial, the investigators initially promised immediate release of IPL data upon completion of the study (August 5, 2021). After this was quickly revealed as empty “virtue signaling,” they then promised to share the data publicly after publication. Almost 2 months now. No data. Numerous interested observers and researchers as well as the funders have asked to see the data. They now state that “IPL data is being held by a third party (ICODA),” and that those interested in obtaining the data can apply to them. A URL provided was dead. The TOGETHER trial website contact gives an auto-reply. I do not believe the data will ever be made public (they would have to do massive manipulation in order to clarify, explain, or defend what we know are fatal flaws in the conduct of the trial. I would be sad if I wasn’t so fucking furious. Bastards. Ed Mills, the Principal Investigator, has also stopped answering questions from interested scientists who have collegial relationships with him. He initially answered a few questions with deliberate misrepresentations and obfuscations and then went dark and has not answered a single follow-up question from anybody since. Quiet as a churchmouse.
I know he and his colleagues are sweating hard. I just don’t think they ever imagined going up against the brilliance and obsessiveness of guys like Alexandros Marinos, Phil Harper, David Wiseman, and David Scheim. Alex was next-level meticulous, devoting dozens of hours to poring over and comparing the timing and recruitment of each study arm’s protocols, dissecting charts and graphs on slides from their public presentations, extensively reading all the supplementary appendices etc. As a result of that herculean effort, Alexandros compiled detailed and extensive evidence that the investigators published data directly conflicting and/or contradicting their public statements. Busted. In order for the data from the paper and the methods in the paper to be consistent with their public statements, they would have to walk back the statements or revise the paper. They are doing neither.
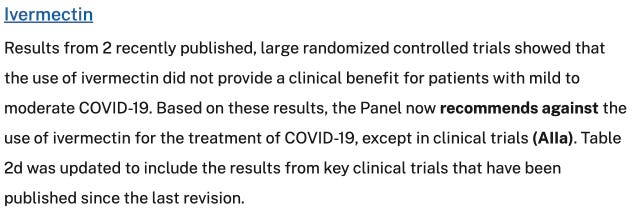
Clearly Big Pharma “gets the win” here. The NIH quietly changed their recommendation back to “do not use outside of a clinical trial”. Read the below and weep for all those getting sick without knowledge or access to effective early treatment.
This post has gone on long enough and I am exhausted with this travesty of a mockery of a sham of a depraved fraud of a trial. But I ain’t giving up the fight. However, if anyone feels like they can stomach more “research fraud porn,” I am including even more crazy stuff from the expert c19early.com group in my addendum below. And if anyone is still convinced this trial was conducted in a good faith effort to find out if ivermectin “really works,” instead of a brazenly fraudulent action by the rapacious pharmaceutical industry, then I got a bridge to sell ya’ as they say. Would be funny except for all the fucking millions of dead people.
Also, check out my other posts in the “Global Disinformation Campaign Against Ivermectin” series:
Part I – Introduction to the Disinformation Playbook
Part II – Exposing the Corrupt Disinformation Campaign on Ivermectin
Part II – Ivermectin – An Attack by New York State’s Attorney General
Part III – Ivermectin – Lawyers Helping Doctors be Doctors
Part IV – Ivermectin – Saturday Night Fight At The Pharmacy
Part IV – Ivermectin – JAMA’s “Diversion Tactic “- the HITECH Trial
Part VII – Op-Ed on Fluvoxamine
Part VIII – Op-Ed on Remdesivir
Part IX – Ivermectin – “The Fix“ of Andrew Hill – Chapter 1
Part X -Ivermectin – “The Fix” of Andrew Hill – Chapter 2
Part XI- Big Pharma’s “Diversion” – The TOGETHER Trial Published in the New England Journal of Medicine
And for those of you looking for more evidence of fraud in this trial, read these telling excerpts from this comprehensive analysis by the c19early.com group:
Delayed >6 months. The paper was delayed over 6 months with no explanation. The companion fluvoxamine arm, completed at the same time, was published Aug 23, 2021. The paper was submitted to NEJM in Sep 2021 [vimeo.com (B)]. COI forms suggest that additional authors were added after submission and the corresponding author changed from Prof. Mills to Dr. Rayner [doyourownresearch.substack.com], whose conflicts include Pfizer, Merck, the Gates Foundation, and the Australian Government.
Data Safety Monitoring Board was not independent. Reviewer 1 of the protocol notes that the DSMC is not independent [gatesopenresearch.org]. Prof. Thorlund is Vice President of the contract research organisation (CRO, Cytel), professor at the sponsoring university, and an author of the protocol. Dr. Häggström is an employee of the CRO. [doyourownresearch.substack.com (C), twitter.com (B)] reveals many other conflicts. Prof. Thorlund has written >100 papers with Prof. Mills. Prof. Singh has written 29 papers with Prof. Mills. Prof. Orbinski has written 9 papers with Prof. Mills. The first version of the web site showed Prof. Mills and Prof. Thorlund as joint leads. Emails pointed to a company MTEK Sciences, founded by Prof. Mills and Prof. Thorlund (MTEK is hypothesized to stand for Mills, Thorlund, Edward, Kristian). MTEK received grants from the Gates Foundation. MTEK also employed Dr. Häggström. MTEK was acquired by Cytel in 2019. Dr. Häggström works for the Gates Foundation. Two members of the DSMC have published a paper with members of a well known anti-ivermectin research group [Thorlund] and Dr. Hill, whose meta analysis has reports of external influence [c19ivermectin.com, c19ivermectin.com (B), twitter.com (C)]. The trial protocol reports that “an independent DSMC will be established, composed of scientists of unrivalled reputation and expertise, without involvement with this research protocol.”
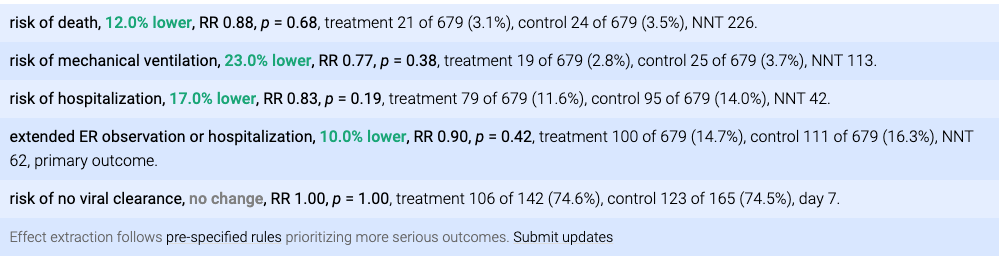
Incorrect conclusion. The conclusion states that ivermectin “did not result in a lower incidence of [hospitalization] or of [ER observation >6hr]”. This is incorrect, hospitalization was 17% lower, which is not statistically significant with the sample size and typical statistical analysis. For the Bayesian analysis the authors use, the ITT probability of superiority for ivermectin was 79.4%, which is a positive result, the opposite of the conclusion.
Bayesian probability of superiority hidden in appendix. The bayesian probability of superiority figure, featured in the main paper for FLV, MET, HCQ, was hidden in the appendix for IVM [twitter.com (W)].
Conflicting target enrollment. There are conflicting target enrollment numbers. The protocol showed 800 patients per arm as of Mar 21, 2021 (after the trial started) [static1.squarespace.com, twitter.com (L)], the co-principal investigator reported 800 per arm in an interview published June 14, 2021 [halifaxexaminer.ca], and the protocol changed to 681 on June 22 [static1.squarespace.com (B)]. However, the trial record from Jan indicates 2724 (681*4) patients [clinicaltrials.gov (C)], suggesting that the 800 goal was later, and was kept for fluvoxamine but reverted for ivermectin. The fluvoxamine arm which started two months earlier was terminated at the same time, and was terminated due to superiority [Reis] after 741/756 patients. Note that Gamma was declining significantly around the termination point, which likely favors improved efficacy if the trial continued, given the late treatment and dosage used.
Reportedly terminated for futility although futility threshold not reached. The trial was reportedly terminated due to futility [twitter.com (M)], however the futility thresholds were 20%, 40% and 60%, and all published probabilities are >60% (ITT 79.4%). Additionally, the fluvoxamine arm did not have the higher 60% threshold, only using 40%. Note the DSMC was not independent as below.
Inconsistent subgroup analysis. The presented subgroup analysis is inconsistent with plans and with the fluvoxamine paper, including not presenting pre-specified subgroups, presenting subgroups that were not pre-specified, presenting different subgroups to the contemporary fluvoxamine paper, and modifying subgroup definitions [twitter.com (P)].
Source – https://pierrekory.substack.com/p/fraudulent-trial-on-ivermectin-published-859?